Abstract
Importance: Contrast-associated acute kidney injury (AKI) is a common complication of coronary angiography and percutaneous coronary intervention (PCI) that has been associated with high costs and adverse long-term outcomes. 造影剂相关的急性肾损伤 (AKI) 是冠状动脉造影和经皮冠状动脉介入治疗 (PCI) 的常见并发症,与高成本和不良的长期结果相关。
Objective: To determine whether a multifaceted intervention is effective for the prevention of AKI after coronary angiography or PCI.确定多方面干预是否能有效预防冠状动脉造影或 PCI 后的 AKI。
Design, setting, and participants: A stepped-wedge, cluster randomized clinical trial was conducted in Alberta, Canada, that included all invasive cardiologists at 3 cardiac catheterization laboratories who were randomized to various start dates for the intervention between January 2018 and September 2019. Eligible patients were aged 18 years or older who underwent nonemergency coronary angiography, PCI, or both; who were not undergoing dialysis; and who had a predicted AKI risk of greater than 5%. Thirty-four physicians performed 7820 procedures among 7106 patients who met the inclusion criteria. Participant follow-up ended in November 2020. 在加拿大阿尔伯塔省进行了一项阶梯楔形整群随机临床试验,其中包括 3 个心导管实验室的所有侵入性心脏病专家,他们被随机分配到 2018 年 1 月至 2019 年 9 月之间的不同干预开始日期。符合条件的患者年龄为 18 岁或 接受非急诊冠状动脉造影、PCI或两者兼有的老年人; 未接受透析的人; 并且预测的 AKI 风险大于 5%。 在符合纳入标准的 7106 名患者中,34 名医生进行了 7820 次手术。 参与者随访于 2020 年 11 月结束。
Interventions: During the intervention period, cardiologists received educational outreach, computerized clinical decision support on contrast volume and hemodynamic-guided intravenous fluid targets, and audit and feedback. During the control (preintervention) period, cardiologists provided usual care and did not receive the intervention. 在干预期间,心脏病专家接受了教育外展、关于对比量和血流动力学指导的静脉输液目标的计算机化临床决策支持,以及审计和反馈。 在控制(干预前)期间,心脏病专家提供常规护理,但未接受干预。
Main outcomes and measures: The primary outcome was AKI. There were 12 secondary outcomes, including contrast volume, intravenous fluid administration, and major adverse cardiovascular and kidney events. The analyses were conducted using time-adjusted models.主要结果是 AKI。 有 12 个次要结果,包括对比剂体积、静脉输液和主要不良心血管和肾脏事件。 使用时间调整模型进行分析。
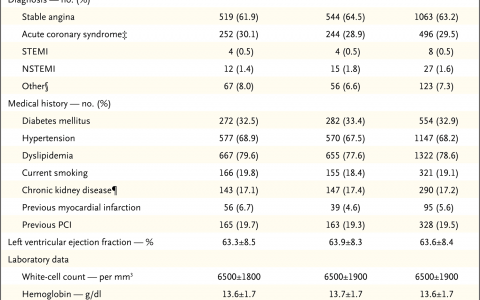
Results: Of the 34 participating cardiologists who were divided into 8 clusters by practice group and center, the intervention group included 31 who performed 4327 procedures among 4032 patients (mean age, 70.3 [SD, 10.7] years; 1384 were women [32.0%]) and the control group included 34 who performed 3493 procedures among 3251 patients (mean age, 70.2 [SD, 10.8] years; 1151 were women [33.0%]). The incidence of AKI was 7.2% (310 events after 4327 procedures) during the intervention period and 8.6% (299 events after 3493 procedures) during the control period (between-group difference, -2.3% [95% CI, -0.6% to -4.1%]; odds ratio [OR], 0.72 [95% CI, 0.56 to 0.93]; P = .01). Of 12 prespecified secondary outcomes, 8 showed no significant difference. The proportion of procedures in which excessive contrast volumes were used was reduced to 38.1% during the intervention period from 51.7% during the control period (between-group difference, -12.0% [95% CI, -14.4% to -9.4%]; OR, 0.77 [95% CI, 0.65 to 0.90]; P = .002). The proportion of procedures in eligible patients in whom insufficient intravenous fluid was given was reduced to 60.8% during the intervention period from 75.1% during the control period (between-group difference, -15.8% [95% CI, -19.7% to -12.0%]; OR, 0.68 [95% CI, 0.53 to 0.87]; P = .002). There were no significant between-group differences in major adverse cardiovascular events or major adverse kidney events. 在按实践组和中心分为 8 个集群的 34 名参与的心脏病专家中,干预组包括 31 名,他们在 4032 名患者中进行了 4327 次手术(平均年龄,70.3 [SD,10.7] 岁;1384 名女性 [32.0%])和对照组包括 34 名患者,他们在 3251 名患者中进行了 3493 次手术(平均年龄,70.2 [SD,10.8] 岁;1151 名女性 [33.0%])。干预期间 AKI 的发生率为 7.2%(4327 次手术后 310 起事件),而在对照组期间为 8.6%(3493 次手术后 299 起事件)(组间差异,-2.3% [95% CI,-0.6% 至-4.1%];优势比 [OR],0.72 [95% CI,0.56 至 0.93];P = .01)。在 12 个预先设定的次要结局中,8 个没有显着差异。在干预期间,使用过多造影剂的手术比例从对照组的 51.7% 降至 38.1%(组间差异,-12.0% [95% CI,-14.4% 至 -9.4%];或,0.77 [95% CI,0.65 至 0.90];P = .002)。符合条件的患者中静脉输液不足的手术比例从对照组的 75.1% 降至干预期间的 60.8%(组间差异,-15.8% [95% CI,-19.7% 至 -12.0 %];OR,0.68 [95% CI,0.53 至 0.87];P = .002)。主要不良心血管事件或主要不良肾脏事件在组间没有显着差异。
Conclusions and relevance: Among cardiologists randomized to an intervention including clinical decision support with audit and feedback, patients undergoing coronary procedures during the intervention period were less likely to develop AKI compared with those treated during the control period, with a time-adjusted absolute risk reduction of 2.3%. Whether this intervention would show efficacy outside this study setting requires further investigation. 在随机接受包括审核和反馈的临床决策支持在内的干预的心脏病专家中,与对照组相比,在干预期间接受冠状动脉手术的患者发生 AKI 的可能性较小,经时间调整的绝对风险降低了 2.3%。 这种干预是否会在该研究环境之外显示出有效性需要进一步调查。
原创文章(本站视频密码:66668888),作者:xujunzju,如若转载,请注明出处:https://zyicu.cn/?p=14145
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫