A 63-year-old otherwise healthy man is discovered to have atrial fibrillation during an evaluation for a viral respiratory infection. He reports that 3 months earlier he began noticing occasional dyspnea on climbing stairs, and this symptom has been persistent for the past month. On physical examination, the body-mass index (BMI; the weight in kilograms divided by the square of the height in meters) is 29, the blood pressure is 142/88mmHg, the pulse is irregular at 120 beats per minute, and there are irregular first and second heart sounds. Electrocardiographic (ECG) evaluation shows atrial fibrillation, normal QRS complexes, and a ventricular rate of 110 beats per minute. How would you evaluate and treat this patient?
一名63岁的健康男子在评估病毒性呼吸道感染时发现心房颤动。据患者描述,3个月前,他开始注意到偶尔在爬楼梯时出现呼吸困难,并且这种症状持续了一个月。体格检查方面,身体质量指数[BMI;体重(公斤)除以身高(米)的平方]为29,血压142/88 mmHg,脉搏不规则,每分钟120次,第一心音和第二心音不规则。心电图检查显示心房颤动,QRS波群正常,心室率为每分钟110次。
The Clinical Problem
In clinical practice, atrial fibrillation is the most common sustained arrhythmia encountered in adults. Among patients in the Framingham Heart Study population, atrial fibrillation developed in 37% after the age of 55 years in those who reached that age. Risk factors include older age, coronary artery disease, male sex, European ancestry, hypertension, obesity, smoking, diabetes mellitus, obstructive sleep apnea, and a family history of atrial fibrillation in a first-degree relative. In a large multi-institutional study, 19% of the patients with newly diagnosed atrial fibrillation had an acute precipitant such as pneumonia or surgery (the two most common precipitants), myocardial infarction, pulmonary embolism, thyrotoxicosis, or alcohol intoxication.
在临床实践中,心房颤动是成人最常见的持续性心律失常。在Framingham心脏研究人群中,37%的患者在55岁以后发生心房颤动。危险因素包括年龄较大、冠状动脉疾病、男性、欧洲血统、高血压、肥胖、吸烟、糖尿病、阻塞性睡眠呼吸暂停和一级亲属心房颤动家族史。在一项大型多机构研究中,19%的新诊断的心房颤动患者有急性诱发因素,如肺炎或手术(两种最常见的诱发因素)、心肌梗死、肺栓塞、甲状腺机能亢进或酒精中毒。
- 房颤与基础心脏病以及死亡、卒中、心力衰竭和痴呆风险增加相关。
- 与房颤风险相关的疾病(包括高血压、高脂血症、糖尿病、睡眠呼吸暂停、肥胖和过量饮酒)的治疗可降低房颤复发的风险。
- 使用是否存在卒中风险因素来估计卒中风险,以确定抗凝是否适用于阵发性或持续性房颤。
- 当房颤持续48小时或更长时间或持续时间未知且计划进行择期复律时,即使不存在卒中风险因素,复律前后也需要一段时间的抗凝治疗。
- 不受控制的心动过速可导致左心室功能恶化。当房颤持续不超过1年或呈阵发性、有症状时,应考虑尝试维持窦性心律。导管消融比抗心律失常药物治疗更有效,尤其是对于阵发性房颤。
Atrial fibrillation is associated with an increased incidence of stroke (by a factor of approximately 4.0 in men and 5.7 in women), heart failure (by a factor of 3.0 in men and 11.0 in women), and dementia that is probably related to strokes and cerebral hypoperfusion (by a factor of 1.4 in a mixed population). Atrial fibrillation increases the risk of death by a factor of 2.4 among men and by a factor of 3.5 among women. In part, this increase reflects the fact that atrial fibrillation is often a marker for underlying heart and vascular disease. However, atrial fibrillation itself probably contributes to adverse outcomes by increasing the risk of stroke, diminishing cardiac performance, and exposing symptomatic patients to therapies that also have risks.
心房颤动与卒中(男性增加约4.0倍,女性增加5.7倍)、心力衰竭(男性增加3.0倍,女性增加11.0倍),以及可能与卒中和脑灌注不足有关的痴呆(混合人群中增加1.4倍)有关。心房颤动使男性死亡风险增加2.4倍,女性增加3.5倍。在某种程度上,这种增长反映了这样一个事实,即心房颤动通常是潜在心脏和血管疾病的一个标志。然而,房颤本身可能会增加卒中风险,降低心脏功能,并使有症状的患者接受同样有风险的治疗,从而可能导致不良后果。
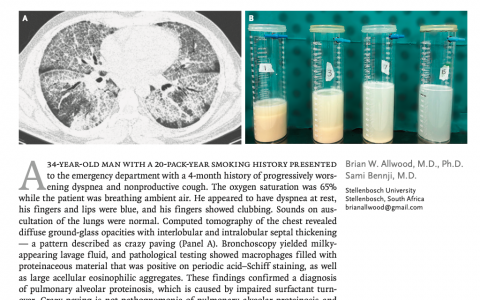
Although the mechanisms are debated and presumably vary among patients, abnormalities of electrophysiological atrial myocytes as well as atrial structural changes, including fibrosis, probably create the electrical substrate that causes atrial fibrillation. The extent and severity of abnormalities increase with age and vary according to the type of atrial fibrillation (Figure 1). Paroxysmal atrial fibrillation occurs in episodes that terminate spontaneously, usually within hours to days. It is often initiated by rapid firing of myocardial triggers in the pulmonary-vein sleeves (Fig. S1 in the Supplementary Appendix, available with the full text of this article at NEJM.org). Persistent atrial fibrillation continues unless it is interrupted by electrical or pharmacologic cardioversion, and it is associated with greater atrial fibrosis than paroxysmal atrial fibrillation. Pulmonary-vein triggers may still initiate the arrhythmia, but additional structural and electrophysiological changes allow atrial fibrillation to persist once it is initiated. Electrical isolation of pulmonary veins alone is less likely to prevent the recurrence of persistent atrial fibrillation than to prevent the recurrence of paroxysmal atrial fibrillation.
尽管机制存在争议,并且可能因患者而异,但电生理心房肌细胞的异常以及包括纤维化在内的心房结构变化,可能是导致心房颤动的电基质。异常的程度和严重程度随着年龄的增长而增加,并随房颤类型而有所不同(图1)。阵发性房颤发作时,通常在数小时至数天内自动终止。
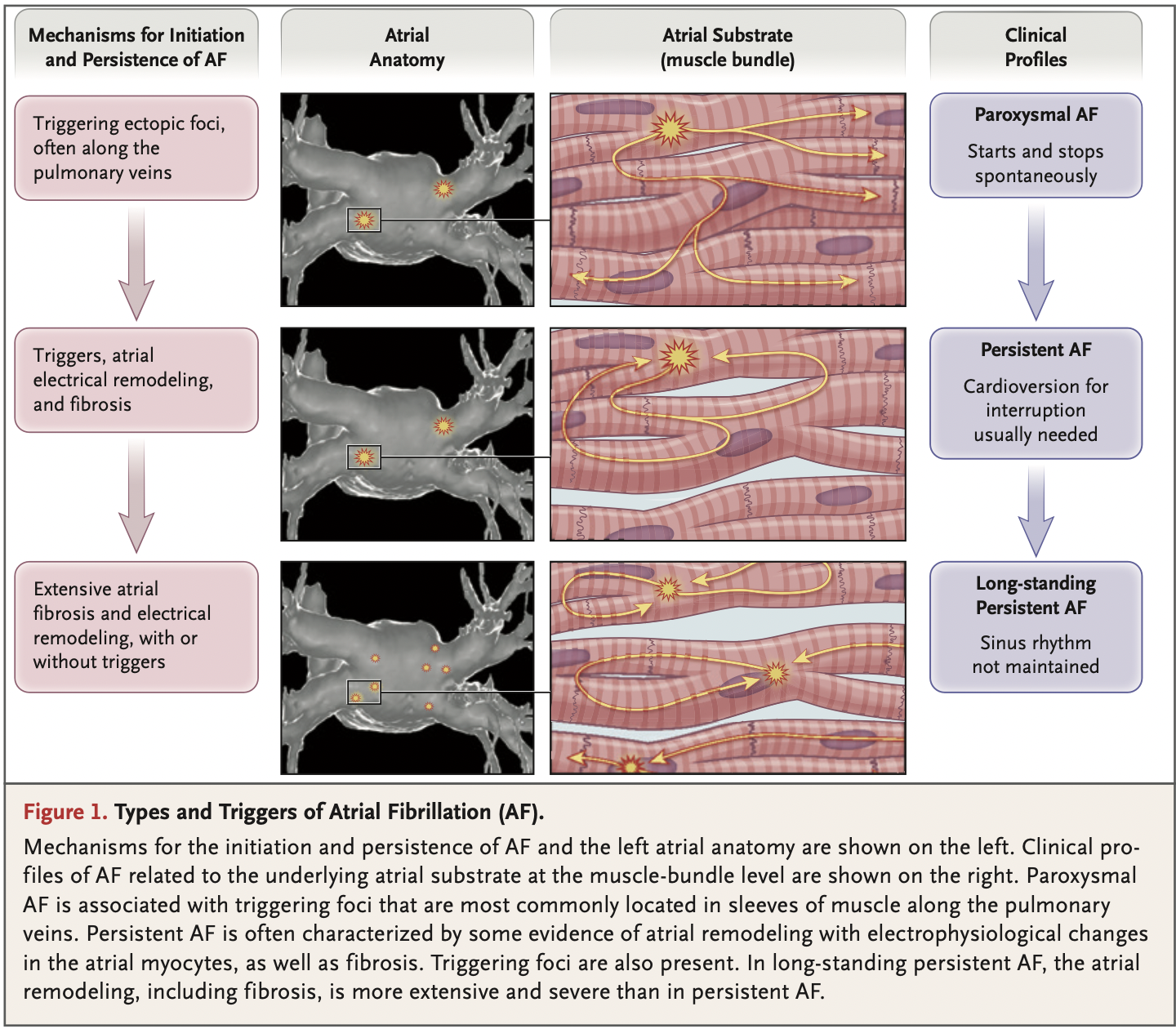
左图:显示了房颤发生和持续的机制以及左房解剖结构。右图:显示了与肌束水平的心房基质相关的心房颤动的临床特征。阵发性房颤与触发病灶有关,这些病灶最常位于沿肺静脉的肌袖中。持续性房颤通常以心房重构、心房肌细胞电生理改变和纤维化为特征。在长期持续性房颤中,心房重构,包括纤维化,比持续性房颤更广泛、更严重。
More than two thirds of patients with recently discovered atrial fibrillation have a paroxysmal pattern, but 5 to 10% per year have progression to persistent atrial fibrillation. Among patients who present with persistent atrial fibrillation and successfully undergo cardioversion, up to 20% have recurrent atrial fibrillation such that it becomes difficult to maintain sinus rhythm.
最近发现的心房颤动患者中,超过三分之二的患者为阵发性,但每年有5%到10%的患者进展为持续性房颤。在持续性房颤并成功转复的患者中,多达20%的患者有房颤复发,从而难以维持窦性心律。
Strategies and Evidence
DIAGNOSIS AND EVALUATION
Symptoms of atrial fibrillation, when present, range from minimal to incapacitating. Atrial fibrillation may cause fatigue, decreased exercise tolerance, and palpitations. Rapid heart rates may cause hypotension, syncope, angina, or pulmonary edema, and emergency treatment may be warranted. Severe manifestations are often associated with acute illness or surgery that leads to increased sympathetic tone and a rapid ventricular rate. Atrial fibrillation can cause a depressed left ventricular ejection fraction that improves or completely reverses after adequate rate control or restoration of sinus rhythm. Although this atrial fibrillation–induced cardiomyopathy usually occurs when the ventricular rate is persistently faster than 110 beats per minute, it may occur at slower rates in some patients.
心房颤动的症状,如果存在,范围从轻微到丧失能力。房颤可能导致疲劳、运动耐力下降和心悸。心率过快可能导致低血压、晕厥、心绞痛或肺水肿,可能需要紧急治疗。严重的症状通常与急性疾病或手术有关,导致交感神经张力增加和心室率加快。房颤可导致左室射血分数下降,在适当的心率控制或窦性心律恢复后改善或完全逆转。虽然这种由房颤引起的心肌病通常在心室率持续高于每分钟110次时发生,但在某些患者中也可能以较慢的速率发生。
An ECG recording that is required for diagnosis reveals QRS complexes that occur at irregular intervals, with variable oscillation of the baseline between beats and no discrete P waves (Figure 1 and Figure 2). Depending on the frequency of symptoms, ambulatory ECG recording may be required for weeks to months in order to establish the diagnosis of paroxysmal atrial fibrillation. Personal ECG recording systems, including small handheld devices and watches, can reveal atrial fibrillation, but an artifact can mimic or obscure the diagnosis, and confirmatory ECG recordings should be obtained.
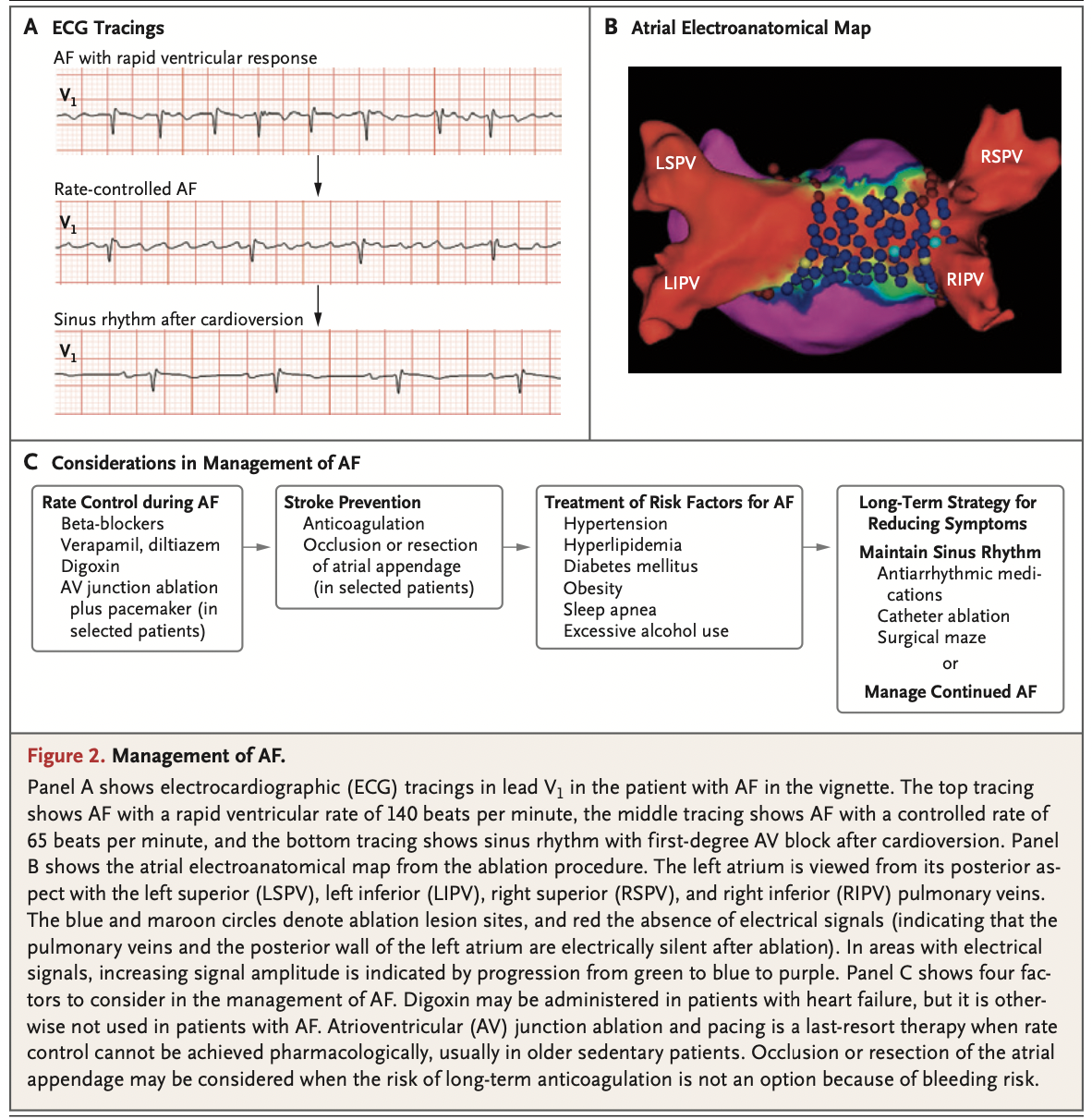
诊断所需的ECG记录显示, QRS波群发生的时间间隔不规律,在每一次搏动之间基线有变化的振荡,没有离散的P波(图1和图2)。根据症状出现的频率不同,可能需要数周至数月的动态心电图记录才能确定阵发性房颤的诊断。个人心电图记录系统,包括小型手持设备和手表,可以显示心房颤动,但伪影可以模拟或掩盖诊断,应该获得确认性心电图记录。
The detection of atrial fibrillation warrants a careful history and physical examination, including measurement of blood pressure, to assess for evidence of predisposing diseases and risk factors and intercurrent illness. Long-term alcohol consumption of more than one drink per day in women and two drinks per day in men has been associated with atrial fibrillation, and binge drinking can precipitate atrial fibrillation. Caffeine consumption has not been shown to increase the incidence of atrial fibrillation. The patient’s blood glucose and thyrotropin levels should be measured.
房颤的评估需要详细的病史和体格检查,包括测量血压,以评估易感疾病、危险因素和合并疾病的证据。女性每天饮酒超过一杯,男性每天饮酒两杯以上的长期饮酒与房颤有关,酗酒会诱发房颤。有证据表明咖啡因的摄入会增加房颤的发生率。应测量患者的血糖和促甲状腺激素水平。
In addition to the ECG and other cardiac monitoring when needed, transthoracic echocardiography is routinely recommended. Screening for sleep-disordered breathing should be performed, and a sleep study should be conducted when the patient’s history is suggestive of sleep apnea.
除了需要时进行心电图和其他心脏监测外,常规推荐使用经胸超声心动图。应进行睡眠呼吸障碍筛查,当患者病史提示有睡眠呼吸暂停时应进行睡眠研究。
TREATMENT
The management of atrial fibrillation has traditionally involved achieving adequate rate control, protection from thromboembolism and stroke, and reduction or elimination of symptoms, as well as the treatment of reversible risk factors (Figure 2). Symptoms may be controlled either by preventing episodes of atrial fibrillation or by slowing the ventricular rate during recurrent atrial fibrillation. In patients in whom atrial fibrillation has developed within the previous year, attempts to maintain sinus rhythm are usually warranted.
房颤的管理传统上包括实现适当的心率控制、防止血栓栓塞和卒中、减轻或消除症状以及可逆危险因素的治疗(图2)。症状可通过预防房颤发作或在房颤复发期间通过减慢心室率来控制。对于前一年发生房颤的患者,通常需要尝试维持窦性心律。
Rate Control
The ventricular rate in atrial fibrillation is an important determinant of hemodynamic consequences and symptoms. Atrioventricular nodal-blocking agents are usually warranted to reduce the ventricular rate. Beta-blockers and nondihydropyridine calcium-channel blockers (verapamil and diltiazem) are first-line therapies. Therapy is tailored to the individual patient and is based on consideration of adverse effects (e.g., beta-adrenergic blockers may aggravate depression, and calcium-channel blockers may aggravate heart failure). Therapy is generally initiated with a beta-blocker at a dose that is adjusted upward, with the aim of controlling symptoms by reducing the heart rate. Although some physicians aim for an average resting heart rate of less than 80 beats per minute, a faster resting rate is acceptable when it is not associated with symptoms, provided that ventricular function remains normal. Calcium-channel blockers may be combined with beta-blockers if the beta-blocker alone is not sufficient, but hypotension can complicate this approach, particularly in older adults. Digoxin slows the resting ventricular rate, but rate control is not usually adequate during exertion. Digoxin has been associated with increased mortality in post hoc analyses of trials involving patients with atrial fibrillation. A low dose of digoxin may be added to other atrioventricular nodal agents to improve rate control, particularly in patients with heart failure. In patients with exertional symptoms, it is important to assess the heart rate response to exertion (e.g., after a brisk walk in the office or with ambulatory monitoring) and to adjust the dose of therapy accordingly.
心房颤动时的心室率是血流动力学后果和症状的重要决定因素。房室结阻滞剂通常用于降低心室率。β-受体阻滞剂和非二氢吡啶类钙通道阻滞剂(维拉帕米和地尔硫卓)是一线治疗药物。治疗是针对不同患者量身定制的,并基于对不良反应的考虑(例如β-肾上腺素受体阻滞剂可能加重抑郁,钙通道阻滞剂可能加重心力衰竭)。治疗一般是用受体阻滞剂开始滴定,剂量上调,目的是通过降低心率来控制症状。虽然一些医生的目标是平均静息心率低于每分钟80次,但如果与症状无关,只要心室功能保持正常,更快的静息心率是可以接受的。如果β受体阻滞剂本身还不够充分,钙通道阻滞剂可以与受β体阻滞剂联合使用,但低血压会使这种方法变得复杂,尤其是在老年人中。地高辛会减慢静息心室率,但在运动过程中心率控制通常不够充分。在涉及心房颤动患者的临床试验的事后分析中,地高辛与死亡率增加有关。
A controlled ventricular response may occur without the use of a rate-controlling agent in healthy patients who have a high vagal tone, as well as in patients with atrioventricular conduction disease. Particularly in older adults, underlying sinus-node disease may lead to symptomatic bradycardia after conversion to sinus rhythm. Permanent pacemaker implantation may be warranted if sinus rhythm is maintained or atrial fibrillation is paroxysmal. Catheter ablation of the atrioventricular node to produce heart block and permanent pacing is a reasonable option for older patients when symptoms due to inadequate rate control continue despite the use of atrioventricular nodal-blocking agents.
在迷走神经张力较高的健康患者和房室传导疾病患者中,在不使用速率控制剂的情况下,可发生控制性心室反应。尤其是在老年人中,潜在的窦房结疾病在转为窦性心律后可能会导致症状性心动过缓。如果维持窦性心律或阵发性心房颤动,可能需要植入永久性起搏器。
Stroke Prevention
Anticoagulation is first-line therapy for prevention of thromboembolism, and its use is guided by estimation of stroke risk according to the CHA2DS2-VASc score (Figure 3). Anticoagulation is indicated for patients who have at least two risk factors (i.e., an estimated stroke risk >2.2% per year) and should be considered for patients who have one risk factor other than female sex (i.e., estimated stroke risk of ≥1.3% per year).
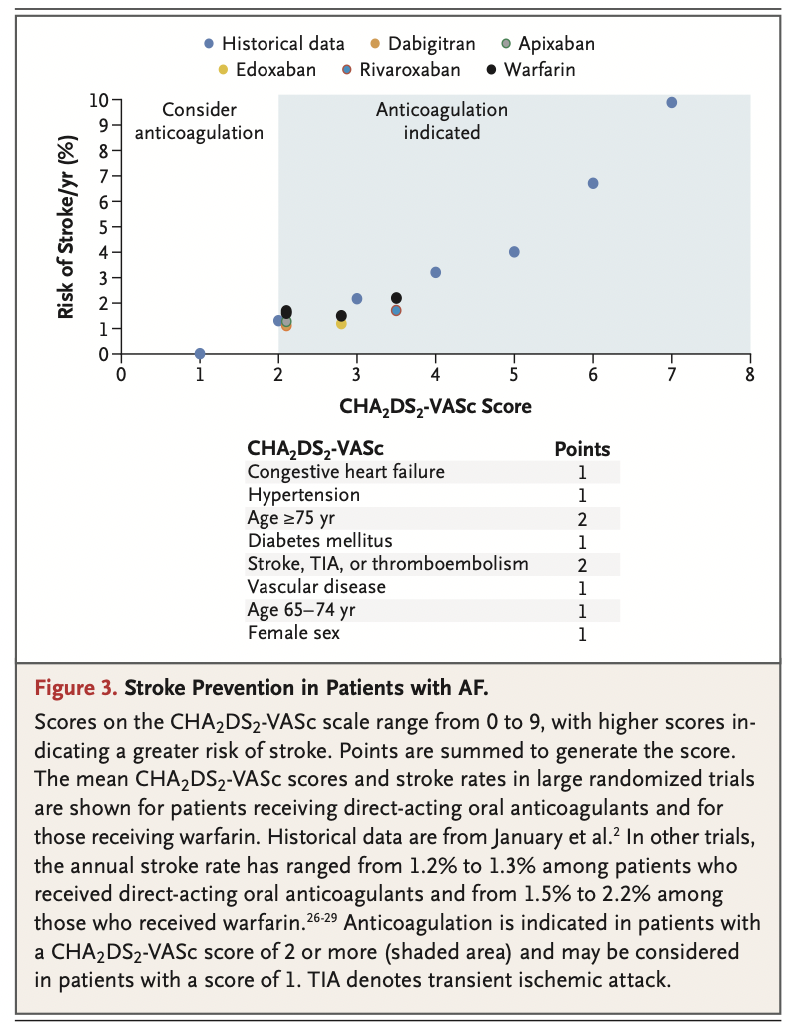
抗凝是预防血栓栓塞的一线疗法,其使用依据是根据CHA2DS2-VASc评分评估卒中风险(图3)。
抗凝适用于至少有两个危险因素(即估计每年卒中风险>2.2%)的患者,并且应该考虑除女性性别外有一个风险因素的患者(即估计每年卒中风险为>1.3%)。
A Cochrane Collaboration review estimated that among patients with atrial fibrillation who had a stroke risk of 4.0% per year, long-term warfarin therapy reduced the risk to 1.4% per year. Several randomized trials have established that direct-acting oral anticoagulants are noninferior to warfarin. A meta-analysis showed that in trials with follow-up ranging from 12 weeks to 2.8 years, the risk of stroke or embolic events was 11% lower among patients who received direct-acting oral anticoagulants than among those who received warfarin; the risk of major bleeding was also reduced (from 5% to 4%) as was the risk of intracranial hemorrhage (from 1.3% to 0.6%). The risk of stroke among patients who received a direct-acting oral anticoagulant was 1.3% to 1.5% per year. In observational studies, apixaban has been associated with less bleeding risk than rivaroxaban. The major route of elimination is renal for all direct-acting oral anticoagulants, with substantial hepatic elimination for apixaban; dosing adjustment is generally needed in patients with renal dysfunction. Unlike warfarin, direct-acting oral anticoagulants do not require repeated laboratory testing to guide dosing and are generally preferred when their greater cost is not prohibitive. Warfarin is still used in patients with mitral stenosis or mechanical heart valves. Aspirin and other antiplatelet therapies alone do not provide adequate protection from stroke in patients with atrial fibrillation.
Cochrane的一项综述估计,在每年卒中风险为4.0%的房颤患者中,长期服用华法林治疗将风险降至每年1.4%。几项随机试验已经证实,直接作用口服抗凝剂不逊于华法林。所有直接作用口服抗凝剂的主要消除途径是肾脏,阿派沙班的主要消除途径是肝脏。肾功能障碍患者通常需要调整剂量。与华法林不同的是,直接作用口服抗凝剂不需要重复的实验室检查来指导剂量,当其成本较高时,通常是首选。华法林仍用于二尖瓣狭窄或机械性心脏瓣膜患者。单用阿司匹林和其他抗血小板疗法并不能充分保护房颤患者免受卒中的危害。
Even in patients who are at low risk for stroke, cardioversion of atrial fibrillation can be followed by atrial thrombus formation and embolization because of delayed recovery of atrial mechanical function. In patients who are at low risk for thromboembolism in whom atrial fibrillation is known to have been present for less than 48 hours, cardioversion is commonly performed without a preceding period of anticoagulation; the reported risk of stroke with this approach is 0.7 to 1.1%, and it occurs mainly in patients with risk factors (Figure 3). When the duration of atrial fibrillation is uncertain or is 48 hours or longer, anticoagulation is recommended for a period of 3 weeks before cardioversion and for another 4 weeks after cardioversion. If cardioversion of atrial fibrillation is warranted sooner, anticoagulation can be initiated and transesophageal echocardiography can be performed. In the absence of left atrial thrombus, cardioversion with continued anticoagulation has a favorable safety profile. After cardioversion, anticoagulation should generally be continued indefinitely in patients with risk factors for stroke.
即使在卒中风险较低的患者中,由于房颤机械功能的延迟恢复,房颤转复后也可能出现房颤血栓形成和栓塞。在血栓栓塞症的低风险患者中,已知存在心房颤动的时间少于48小时,通常在没有抗凝的情况下进行心脏复律;据报道,采用这种方法发生卒中的风险为0.7-1.1%,主要发生在有危险因素的患者(图3)。当房颤持续时间不确定或为48小时或更长时间时,建议在复律前抗凝3周,复律后再抗凝4周。如果需要更早的房颤复律,可以开始抗凝治疗,并进行经食管超声心动图检查。在不存在左心房血栓的情况下,持续抗凝复律具有良好的安全性特征。复律后,有脑卒中危险因素的患者一般应无限期继续抗凝治疗。
Maintenance of Sinus Rhythm
The decision regarding whether to pursue maintenance of sinus rhythm is shared between the patient and physician; this decision is informed by the effect of atrial fibrillation on the patient’s quality of life and by the risks and toxic effects of therapies. Many patients with paroxysmal atrial fibrillation or recently recognized persistent atrial fibrillation have symptoms and want to receive therapy, but some patients with persistent atrial fibrillation adapt without realizing that the arrhythmia is causing a reduction in their activity. For newly recognized asymptomatic atrial fibrillation, an attempt at cardioversion and maintenance of sinus rhythm is often reasonable to assess the symptomatic effect of atrial fibrillation, which then informs further treatment. The large, randomized Early Treatment of Atrial Fibrillation for Stroke Prevention Trial (EAST-AFNET 4) trial compared early rhythm control (with antiarrhythmic drugs or catheter ablation) with usual care in patients who had atrial fibrillation that was diagnosed within 1 year before enrollment and other cardiovascular disease or stroke risk factors. The early rhythm-control strategy was associated with a significantly lower rate of the composite of death from cardiovascular causes, stroke, or hospitalization for heart failure or acute coronary syndrome (by 1.1 events per 100 person years; a 22% reduction), without an increase in the number of nights spent in the hospital. Serious adverse events related to treatment occurred in 4.9% of the patients in the early rhythm-control group; the most common serious adverse event in that group was drug-induced bradycardia (in 1.0% of the patients).
是否维持窦性心律的决定由患者和医生共同决定;这一决定是由房颤对患者生活质量的影响以及治疗的风险和毒性决定的。许多阵发性房颤或近期确诊的持续性房颤患者有症状并希望接受治疗,但部分持续性房颤患者已经适应,却没有意识到心律失常正在导致其活动减少。对于新发现的无症状性房颤患者,尝试转复和维持窦性心律通常是合理的,以评估其房颤的症状效应,然后告知下一步治疗。早期节律控制策略与心血管原因、卒中或因心力衰竭或急性冠状动脉综合征住院的复合死亡率显著降低(每100人年减少1.1个事件,减少22%)相关。早期节律控制组有4.9%的患者发生与治疗相关的严重不良事件,其中最常见的严重不良事件为药物诱发的心动过缓(1.0%)。
Continued therapy with a beta-blocker may reduce episodes of atrial fibrillation in some patients, but it is less effective than antiarrhythmic drugs; atrial fibrillation has been reported to recur in 43 to 67% of patients who receive beta-blockers. Reductions in the frequency and duration of atrial fibrillation episodes are often reasonable goals if they improve symptoms. Adverse effects and contraindications (Table 1) are important considerations in drug selection. Several agents have been linked to an increased risk of death among patients with structural heart disease (e.g., flecainide, propafenone, and d-sotalol) or heart failure (dronedarone). Flecainide, propafenone, sotalol, and dofetilide are options for patients who do not have structural heart disease. Patients who receive sotalol and dofetilide must be monitored closely for prolongation of the corrected QT interval, which can lead to potentially fatal ventricular tachycardia (torsades de pointes). This risk is increased among women (because the QT interval is longer in women than in men), among patients with renal insufficiency or bradycardia, and among those who are taking other drugs that prolong the QT interval or alter antiarrhythmic drug absorption or elimination. Amiodarone is a highly effective antiarrhythmic drug; however, owing to several potential long-term toxic effects, long-term use should be avoided if possible.
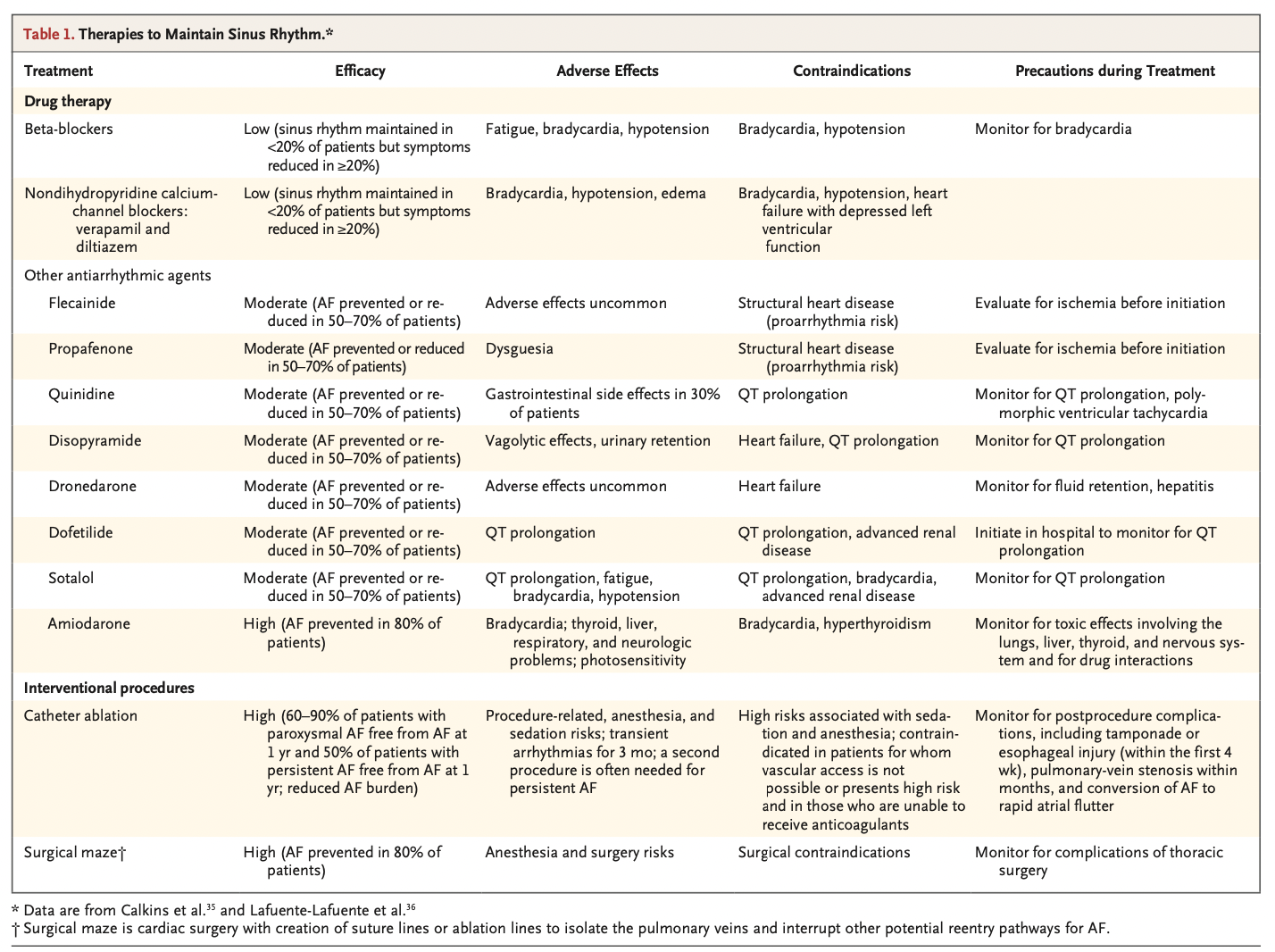
继续使用β受体阻滞剂治疗可能会减少一些患者的房颤的发作,但效果不如抗心律失常药物;据报道,在使用受体阻滞剂的患者中,房颤复发率为43-67%。如果能改善症状,减少房颤发作的频率和持续时间通常是合理的目标。不良反应和禁忌症(表1)是药物选择的重要考虑因素。有几种药物与结构性心脏病(如氯卡尼、普罗帕酮和索他洛尔)或心力衰竭(决奈达隆)患者死亡风险增加有关。必须密切监测接受索他洛尔和多非利特的患者是否出现校正QT间期延长,这可能导致潜在致死性室性心动过速(尖端扭转型室性心动过速)。这种风险在女性(因为女性的QT间期比男性长)、肾功能不全或心动过缓患者以及正在服用其他延长QT间期或改变抗心律失常药物吸收或消除的药物的患者中增加。胺碘酮是一种高效抗心律失常药物;然而,由于几种潜在的长期毒性作用,如果可能,应避免长期使用。
Catheter ablation that is performed with the use of radiofrequency or cryotherapy is more effective than antiarrhythmic drug therapy for maintaining sinus rhythm in patients with paroxysmal atrial fibrillation. Two recent randomized trials compared cryoablation with antiarrhythmic medication in patients with primarily paroxysmal atrial fibrillation. Symptomatic atrial fibrillation recurred by 1 year after a 90-day “blanking period” (i.e., the first 90 days after the index ablation) in 11.0% of the patients who underwent ablation and in 26.2% of those who received antiarrhythmic drugs in one trial. The percentage of patients with treatment success at 1 year was 74.6% in the ablation group and 45.0% in the drug-therapy group in the other trial. Therapies for maintenance of sinus rhythm are generally less effective in patients with persistent atrial fibrillation than in those with paroxysmal atrial fibrillation. In the randomized Catheter Ablation vs. Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) trial, 57% of the patients had persistent atrial fibrillation at trial entry; after 48.5 months of follow-up, only 16% of the patients in the ablation group had persistent atrial fibrillation, as compared with 26% in the drug-therapy group. The most common procedure-related adverse events were associated with vascular access (in 3.9% of the patients); serious complications included cardiac perforation with tamponade (in 0.8%), phrenic-nerve injury (in 0.1%), and transient ischemic attacks from cerebral emboli (in 0.3%). An expert consensus statement noted that procedure-related death occurs in fewer than 1 in 1000 patients. Uncommon late complications include pulmonary-vein stenosis and left atrial esophageal fistula (in 0.02 to 0.11% of patients). The latter manifests 1 to 4 weeks after ablation with a clinical syndrome resembling endocarditis and is fatal without prompt recognition and emergency surgery. During the first 3 months after ablation of atrial fibrillation, atrial tachycardia or atrial flutter occurs in up to 50% of patients and often resolves spontaneously, although antiarrhythmic drug therapy or cardioversion may be warranted. During longer follow-up, atrial fibrillation recurs in 15 to 50% of patients owing to lack of durability of the ablation lesion or the development of a new source of atrial fibrillation. Patients with reductions in atrial fibrillation burden and symptoms do not necessarily have to undergo a repeat procedure.
在阵发性房颤患者中,使用射频或冷冻疗法进行的导管消融在维持窦性心律方面比抗心律失常药物治疗更有效。最近的两项随机试验在原发性阵发性房颤患者中比较了冷冻消融与抗心律失常药物。在一项试验中,11.0%接受消融术的患者和26.2%接受抗心律失常药物治疗的患者在90天“空白期”后1年时(即首次消融术后的前90天)症状性房颤复发。在另一项试验中,消融组和药物治疗组在1年时治疗成功的患者百分比分别为74.6%和45.0%。持续性房颤患者维持窦性心律的治疗通常不如阵发性房颤患者有效。在随机导管消融与抗心律失常药物治疗房颤(CABANA)试验中,57%的患者在试验入组时患有持续性房颤;随访48.5个月后,消融组只有16%的患者出现持续性房颤,而药物治疗组为26%。最常见的手术相关不良事件与血管通路相关(3.9%的患者);严重并发症包括心脏穿孔伴心包填塞(0.8%)、膈神经损伤(0.1%)和短暂性脑缺血发作(0.3%)。专家共识声明指出,手术相关死亡的发生率低于1/1000。不常见的晚期并发症包括肺静脉狭窄和左心房食管瘘(0.02%-0.11%的患者)。后者在消融后1~4周表现为类似心内膜炎的临床综合征,如不及时识别和急诊手术是致命的。在房颤消融术后的前3个月内,高达50%的患者发生房性心动过速或房扑,通常可自行消退,但可能需要抗心律失常药物治疗或复律。在长期随访期间,15%至50%的患者由于消融病变缺乏持久性或出现新的房颤来源而复发房颤。房颤负荷和症状降低的患者不一定必须接受重复手术。
Maintenance of sinus rhythm is improved by the treatment of modifiable risk factors. A randomized trial involving 150 patients with atrial fibrillation showed that the addition of an intensive weight loss program to other therapies (including treatment and counseling for hypertension, sleep apnea, alcohol consumption, hyperlipidemia, and diabetes mellitus) resulted in weight loss as well as less atrial fibrillation and fewer symptoms of atrial fibrillation than the standard intervention. A randomized trial involving patients with atrial fibrillation who consumed more than 10 standard drinks (with 1 standard drink containing approximately 12 g of pure alcohol) per week showed that those assigned to abstain from alcohol (average consumption, ≤2 drinks per week) had a lower atrial fibrillation burden during the following 6 months than those assigned to the control group. A recent scientific statement by the American Heart Association suggested a goal of a 10% reduction in weight for patients with a BMI of 28 or higher, along with routine exercise and management of diabetes, hyperlipidemia, and sleep apnea and moderation of alcohol consumption.
通过治疗可改变的风险因素可改善窦性心律的维持。一项涉及150例房颤患者的随机试验表明,在其他疗法(包括高血压、睡眠呼吸暂停、饮酒、高脂血症的治疗和咨询,和糖尿病)导致体重减轻以及比标准干预更少的房颤和更少的房颤症状。一项涉及房颤患者的随机试验表明,那些被分配戒酒(平均饮酒量,每周≤2次)在接下来的6个月内房颤负荷低于对照组。美国心脏协会最近的一项科学声明提出,对于BMI为28或更高的患者,目标是降低10%的体重,同时进行常规运动和管理糖尿病、高脂血症、睡眠呼吸暂停和适度饮酒。
Guidelines
Guidelines for the management of atrial fibrillation have been written collaboratively by the American College of Cardiology, American Heart Association, and Heart Rhythm Society, the European Society of Cardiology, and the Canadian Cardiovascular Society. Our recommendations are generally concordant with these guidelines.
美国心脏病学会、美国心脏协会和心脏节律学会、欧洲心脏病学会和加拿大心血管学会共同编写了心房颤动管理指南。我们的建议与这些指南大体上是一致的。
Areas of Uncertainty
Data on the effects of strategies to maintain sinus rhythm on the overall risk of death are lacking. Recent randomized trials have suggested that the risk of death may be decreased among patients in whom the sinus rhythm is maintained early after the diagnosis of atrial fibrillation and in those with depressed left ventricular function who are candidates for and who undergo ablation.
关于维持窦性心律的策略对总体死亡风险的影响的数据缺乏。最近的随机试验表明,房颤诊断后早期保持窦性心律的患者以及接受消融治疗的左心室功能低下的患者的死亡风险可能会降低。
Among some patients with atrial fibrillation who are thought to be in sinus rhythm, episodes of atrial fibrillation may go undetected and the risk of stroke appears to be increased. Safe strategies for determining whether patients can discontinue anticoagulation when sinus rhythm is maintained require further definition. Data are needed to inform the outcomes of occlusion or resection of the left atrial appendage, particularly in patients in whom anticoagulation poses high risks.
在一些被认为是窦性心律的心房颤动患者中,心房颤动的发作可能未被发现,卒中的风险似乎增加了。在维持窦性心律的情况下,确定患者是否可以停止抗凝治疗的安全策略需要进一步确定。需要数据来告知封堵或切除左心耳的结果,尤其是在抗凝风险很高的患者中
Conclusions and Recommendations
For a patient such as the one described in the vignette who has newly recognized atrial fibrillation, we would obtain serum electrolyte, creatinine, and thyrotropin levels; identify and treat reversible risk factors; and initiate anticoagulation with a direct-acting oral anticoagulant and therapy with a beta-blocker (adjusting the dose to achieve rate control). Further evaluation would include echocardiography and assessment of possible coronary artery disease with stress testing or angiography. We would perform direct-current cardioversion after a 4-week course of anticoagulation. If atrial fibrillation recurred, decisions regarding further therapy would be guided by symptoms, risks, and benefits and would include consideration of catheter ablation to maintain sinus rhythm.
对于像片段中描述的新发现房颤的患者,我们将获取血清电解质、肌酐和促甲状腺素水平;识别和治疗可逆的危险因素;使用直接口服抗凝剂开始抗凝,并使用β受体阻滞剂进行治疗(调整剂量以实现心率控制)。进一步的评估将包括超声心动图和通过负荷测试或血管造影评估可能的冠状动脉疾病。我们将在4周的抗凝疗程后进行直流电复律。如果房颤复发,进一步治疗的决定将根据症状、风险和益处来指导,并将包括考虑导管消融以维持窦性心律。
特别申明:本文为转载文章,转载自N Engl J Med 2021; 384:353-361,不代表贪吃的夜猫子立场,如若转载,请注明出处:https://www.nejm.org/doi/full/10.1056/NEJMcp2023658
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫