Abstract
Objectives: The Australia and New Zealand Intensive Care Society (ANZICS) Adult Patient Database (APD) has been operational for 3 decades. It is important to understand how mortality outcomes have changed across diagnostic groups over time to facilitate the planning of future healthcare resources. We evaluated the trends in risk-adjusted mortality for ICU patients over the last 30 years.澳大利亚与新西兰重症监护协会(ANZICS)成人患者数据库(APD)已运行三十年。了解不同诊断组患者的死亡率随时间的变化趋势,对未来医疗资源配置的规划至关重要。本研究评估了过去三十年重症监护病房(ICU)患者经风险调整后的死亡率变化趋势。
Design: A retrospective cohort study.回顾性队列研究。
Setting: All ICUs in Australia and New Zealand that contributed data to the ANZICS APD from January 1993 to December 2022.1993年1月至2022年12月期间,向ANZICS APD数据库提交数据的澳大利亚和新西兰所有ICU。
Patients: Adult patients (≥ 16 yr) admitted to Australian and New Zealand ICUs.澳大利亚和新西兰ICU收治的成年患者(≥16岁)。
Interventions: None.无。
Measurements and main results: The final cohort included 2,838,654 patients from 209 ICUs. Compared with the first decade patients admitted during the final decade of the study were older (60.0 yr [18.2 yr] vs. 62.0 yr [17.8 yr]), more often had a least one major comorbidity (23.2% vs. 25.2%), and had higher Acute Physiology and Chronic Health Evaluation III scores (45.6 [28.1] vs. 50.9 [24.1]). The five diagnostic groups with the highest mortality rates were cardiac arrest (53.6%), stroke and intracranial hemorrhage (34.8%), subarachnoid hemorrhage (21.2%), pneumonia (19.2%), and sepsis (19%). Risk-adjusted mortality decreased until 2010 but then plateaued. Cardiac arrest saw the greatest improvement in risk-adjusted mortality between the third vs. first study decades (odds ratio [OR], 0.82 [0.81-0.83]), while pneumonia saw the least (OR, 0.87 [0.87-0.88]). The pattern of improvement for most diagnostic groups were similar; however, mortality from stroke and intracranial hemorrhage continued to improve, whereas mortality from cardiac arrest appears to have increased over the past 10 years.最终队列纳入来自209个ICU的2,838,654例患者。与研究最初十年相比,研究最后十年收治的患者年龄更大(60.0岁[标准差18.2岁] vs. 62.0岁[标准差17.8岁]),合并至少一种主要基础疾病的比例更高(23.2% vs. 25.2%),急性生理与慢性健康评估Ⅲ(APACHE III)评分也更高(45.6分[标准差28.1分] vs. 50.9分[标准差24.1分])。死亡率最高的五个诊断组依次为:心脏骤停(53.6%)、卒中与颅内出血(34.8%)、蛛网膜下腔出血(21.2%)、肺炎(19.2%)和脓毒症(19.0%)。经风险调整后的死亡率在2010年前持续下降,此后趋于平稳。心脏骤停的风险调整死亡率在研究的第三个十年与第一个十年之间改善最为显著(比值比[OR] 0.82 [95%置信区间 0.81–0.83]),而肺炎的改善幅度最小(OR 0.87 [0.87–0.88])。大多数诊断组的改善趋势相似;但卒中与颅内出血的死亡率持续下降,而心脏骤停的死亡率在过去十年中似乎有所上升。
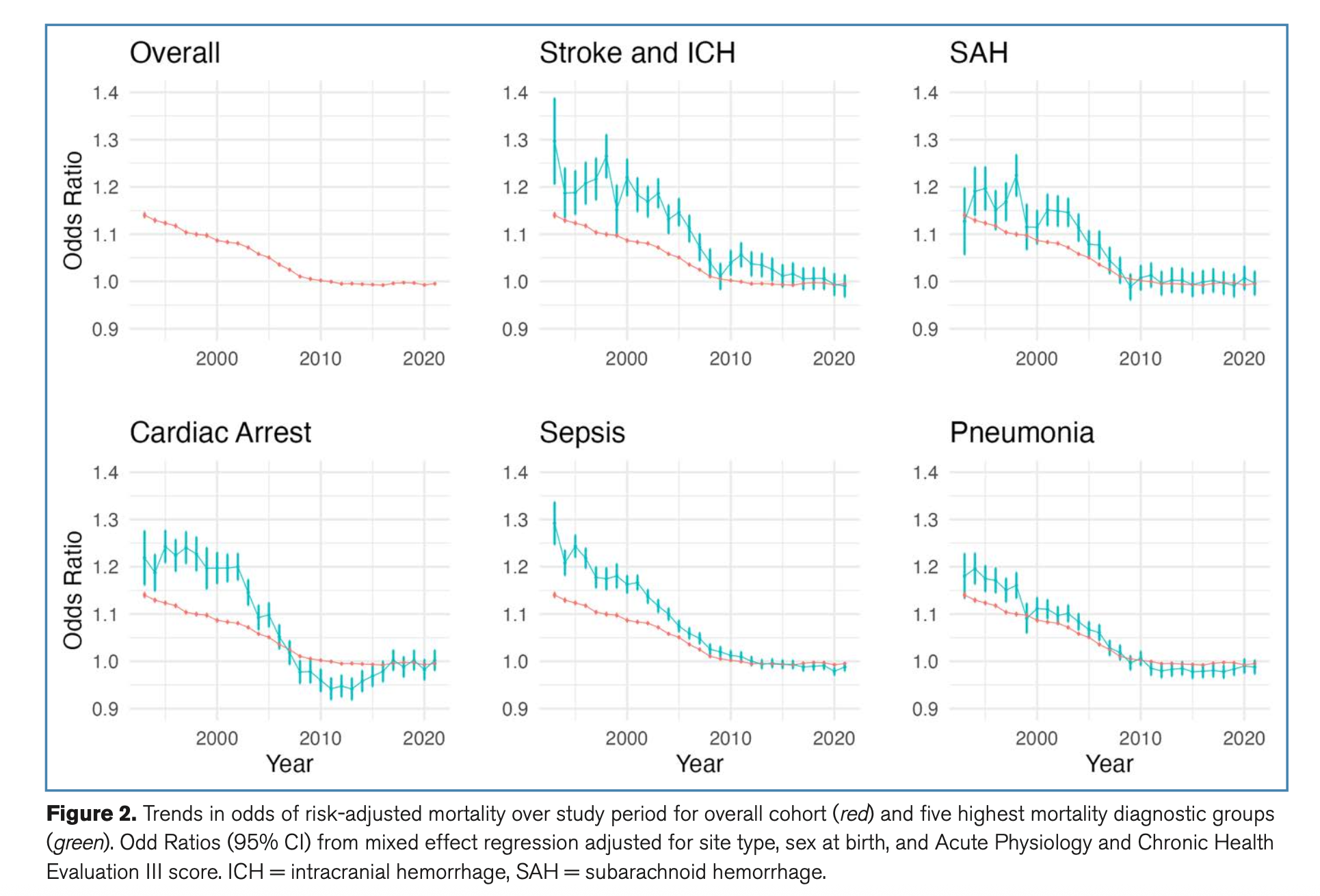
Conclusions: There have been substantial improvements in risk-adjusted mortality among ICU patients over the past 30 years; however, this improvement has plateaued recently. The reasons for this plateau warrant further investigation. 过去三十年间,ICU患者的经风险调整后死亡率显著改善,但近期这一改善趋势已趋于平稳。这种平台期现象的原因值得进一步研究。
原创文章(本站视频密码:66668888),作者:xujunzju,如若转载,请注明出处:https://zyicu.cn/?p=20642
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫