BACKGROUND
Endovascular therapy for acute ischemic stroke is generally avoided when the in- farction is large, but the effect of endovascular therapy with medical care as com- pared with medical care alone for large strokes has not been well studied.
梗死核心较大时,一般避免对急性缺血性卒中进行血管内治疗,但对于大核心梗死卒中,血管内治疗联合药物治疗与单纯药物治疗的疗效比较尚未经过充分研究。
METHODS
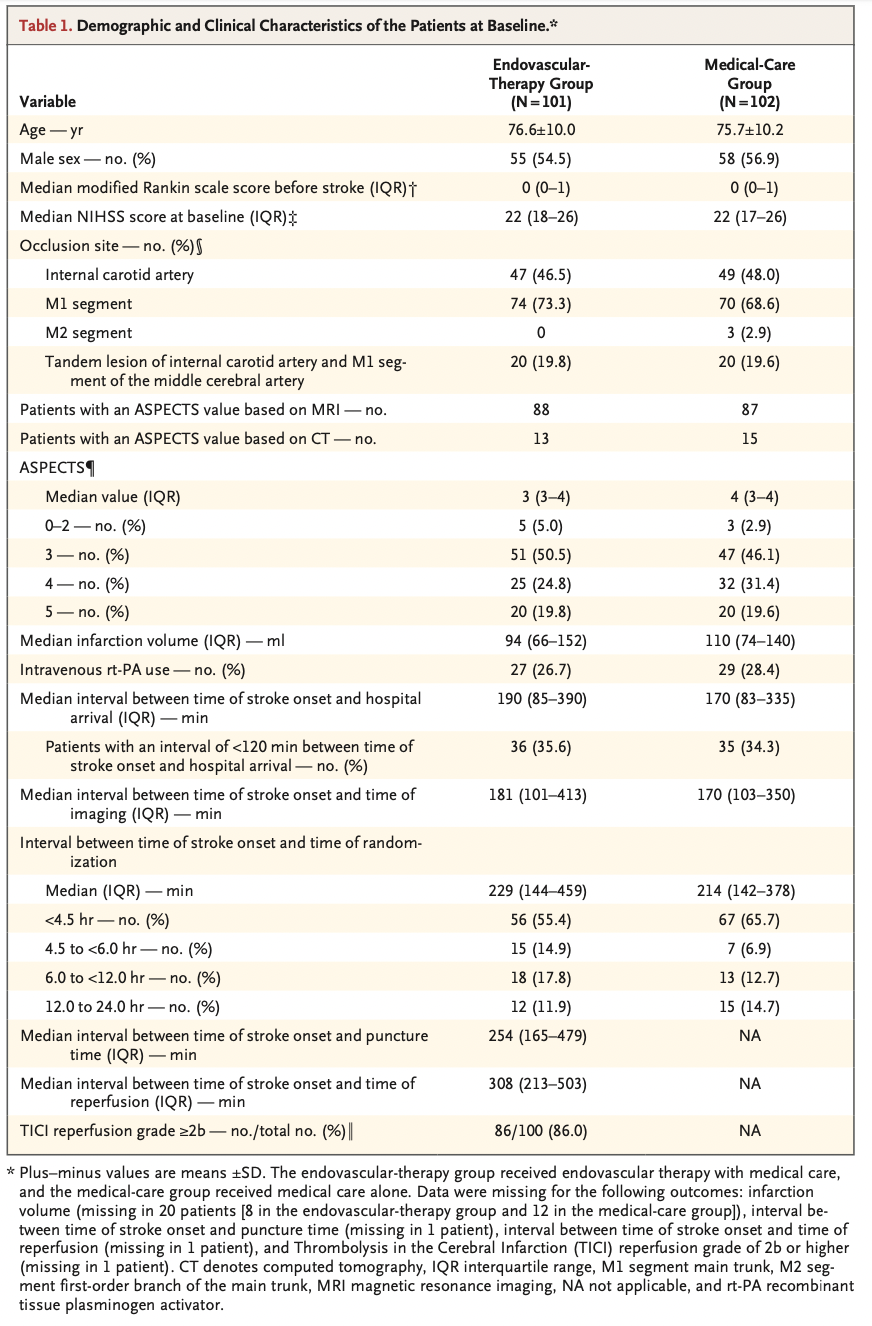
We conducted a multicenter, open-label, randomized clinical trial in Japan involving patients with occlusion of large cerebral vessels and sizable strokes on imaging, as indicated by an Alberta Stroke Program Early Computed Tomographic Score (ASPECTS) value of 3 to 5 (on a scale from 0 to 10, with lower values indicating larger infarction). Patients were randomly assigned in a 1:1 ratio to receive endovas- cular therapy with medical care or medical care alone within 6 hours after they were last known to be well or within 24 hours if there was no early change on fluid- attenuated inversion recovery images. Alteplase (0.6 mg per kilogram of body weight) was used when appropriate in both groups. The primary outcome was a modified Rankin scale score of 0 to 3 (on a scale from 0 to 6, with higher scores indicating greater disability) at 90 days. Secondary outcomes included a shift across the range of modified Rankin scale scores toward a better outcome at 90 days and an improve- ment of at least 8 points in the National Institutes of Health Stroke Scale (NIHSS) score (range, 0 to 42, with higher scores indicating greater deficit) at 48 hours.
我们在日本开展了一项多中心、开放标签、随机临床试验,试验纳入影像学检查显示脑部大血管闭塞的大核心梗死卒中患者,即Alberta卒中项目早期CT评分(Alberta Stroke Program Early Computed Tomographic Score,ASPECTS)值为3~5分(0~10分量表,数值较低表示梗死核心较大)。我们以1∶1的比例将患者随机分组,两组均在最后已知健康状况良好后6小时内或24小时内(如果液体衰减反转恢复图像无早期变化)接受治疗,分别接受血管内治疗+药物治疗或单纯药物治疗。适合的情况下,对两组患者使用了阿替普酶(0.6 mg/kg体重)治疗。主要结局是90日时的改良Rankin量表评分为0~3分(量表评分范围为0~6分,评分较高表示残疾较严重)。次要结局包括90日时改良Rankin量表评分向更好结局变化,以及48小时美国国立卫生研究院卒中量表(National Institutes of Health Stroke Scale,NIHSS)评分(范围,0~42分,评分较高表示神经功能缺损较严重)改善至少8分。
RESULTS
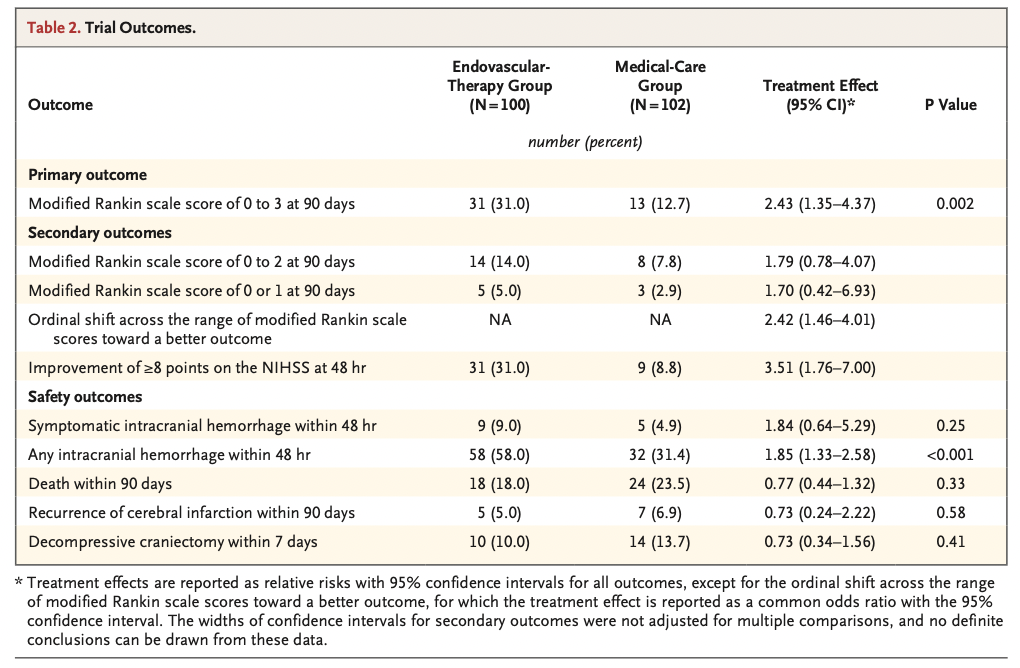
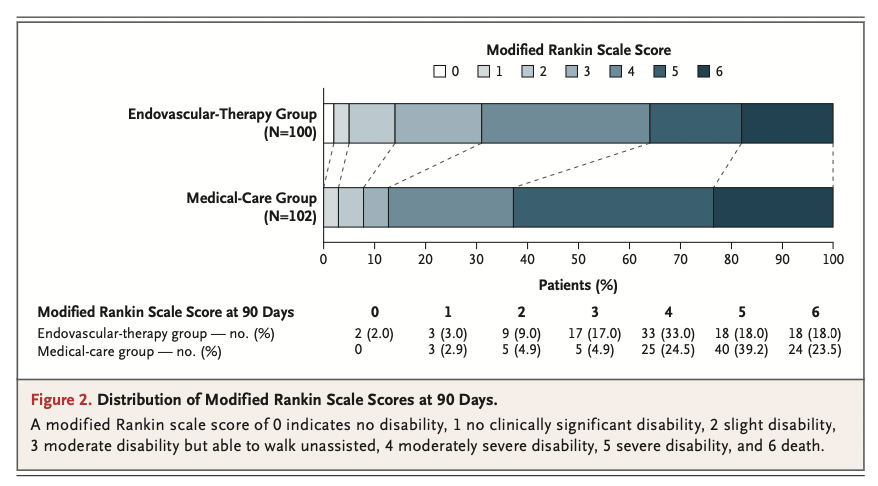
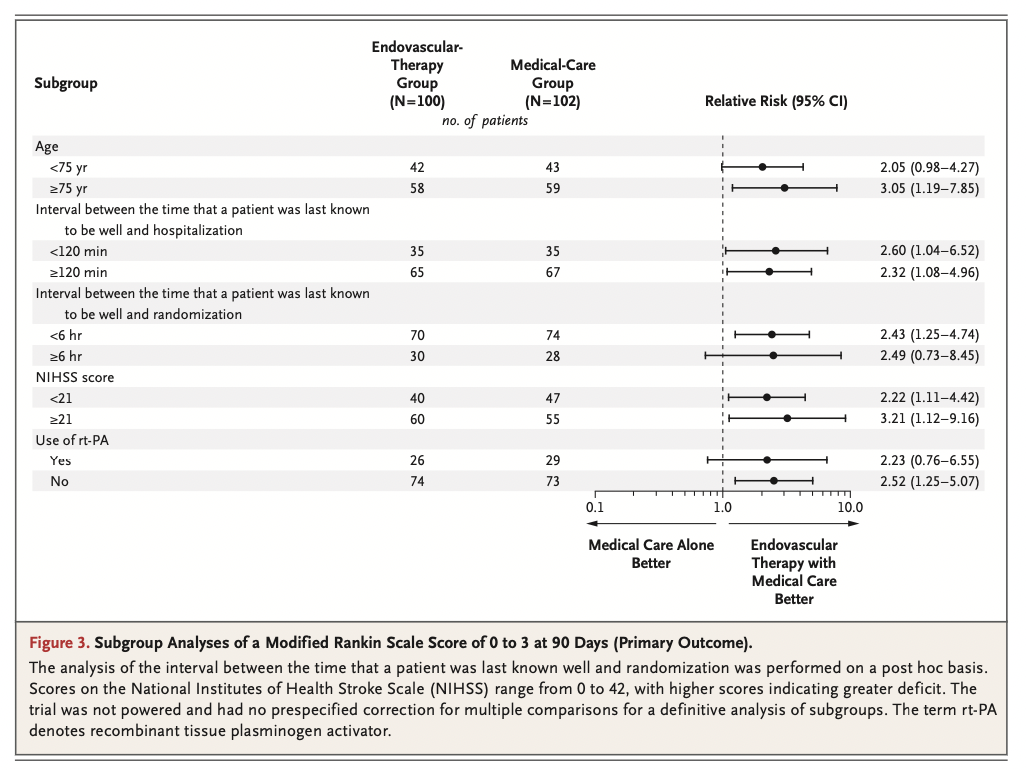
A total of 203 patients underwent randomization; 101 patients were assigned to the endovascular-therapy group and 102 to the medical-care group. Approximately 27% of patients in each group received alteplase. The percentage of patients with a modified Rankin scale score of 0 to 3 at 90 days was 31.0% in the endovascular- therapy group and 12.7% in the medical-care group (relative risk, 2.43; 95% con- fidence interval [CI], 1.35 to 4.37; P=0.002). The ordinal shift across the range of modified Rankin scale scores generally favored endovascular therapy. An improve- ment of at least 8 points on the NIHSS score at 48 hours was observed in 31.0% of the patients in the endovascular-therapy group and 8.8% of those in the medical- care group (relative risk, 3.51; 95% CI, 1.76 to 7.00), and any intracranial hemor- rhage occurred in 58.0% and 31.4%, respectively (P<0.001).
共计203例患者接受了随机分组;101例患者被分配至血管内治疗组,102例患者被分配至药物治疗组。每组约27%的患者接受了阿替普酶治疗。在血管内治疗组和药物治疗组中,90日改良Rankin量表评分为0~3分的患者百分比分别为31.0%和12.7%(相对危险度,2.43;95%置信区间[CI],1.35~4.37;P=0.002)。在改良Rankin量表评分变化情况方面,一般血管内治疗组较优。血管内治疗组31.0%的患者和药物治疗组8.8%的患者的48小时NIHSS评分改善至少8分(相对危险度,3.51;95% CI,1.76~7.00),两组的颅内出血发生率分别为58.0%和31.4%(P<0.001)。

CONCLUSIONS
In a trial conducted in Japan, patients with large cerebral infarctions had better functional outcomes with endovascular therapy than with medical care alone but had more intracranial hemorrhages. (Funded by Mihara Cerebrovascular Disorder Research Promotion Fund and the Japanese Society for Neuroendovascular Therapy; RESCUE-Japan LIMIT ClinicalTrials.gov number, NCT03702413.)
在日本此项纳入大核心梗死患者的试验中,血管内治疗组的功能结局优于单纯药物治疗组,但前者的颅内出血较多(由三原脑血管疾病研究促进基金[Mihara Cerebrovascular Disorder Research Promotion Fund]和日本脑神经血管内治疗学会[Japanese Society for Neuroendovascular Therapy]资助,RESCUE-Japan LIMIT在ClinicalTrials.gov注册号为NCT03702413)。
特别申明:本文为转载文章,转载自NEJM医学前沿,不代表贪吃的夜猫子立场,如若转载,请注明出处:http://www.nejmqianyan.cn/article-info?permalinks=YXQYoa2118191
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫