Abstract
Background
The role of intra-aortic balloon pump (IABP) combined with venoarterial extracorporeal membrane oxygenation (VA-ECMO) in patients with cardiogenic shock (CS) remains unclear. This study investigated the effect of applying IABP for left ventricle (LV) unloading after VA-ECMO on reducing mortality in patients with CS.主动脉内球囊泵(IABP)与静脉-动脉体外膜氧合(VA-ECMO)联合在心源性休克(CS)患者中的使用效果尚不明确。本研究调查了在VA-ECMO后应用IABP进行左心室(LV)减负荷以降低CS患者死亡率的效果。
Methods
Data from 5,492 consecutive patients with CS treated with VA-ECMO between January 2017 and July 2023 were collected from the CSECLS registry. The primary outcome was in-hospital mortality. The secondary outcomes included 30-day mortality, survival on VA-ECMO, and various complications. The association between the application of IABP after VA-ECMO and in-hospital outcomes was assessed.从2017年1月至2023年7月,从中国体外生命支持(CSECLS)注册数据库收集了5492例连续接受VA-ECMO治疗的CS患者的数据。主要结果是住院死亡率。次要结果包括30天死亡率、VA-ECMO存活率和各种并发症。评估了VA-ECMO后应用IABP与住院结果之间的关联。
Results
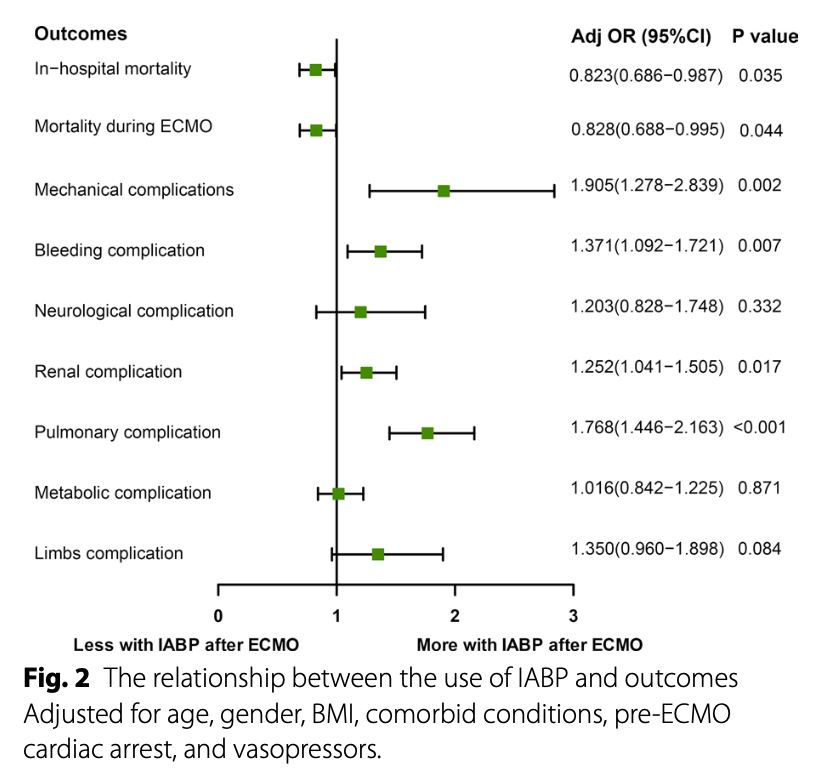
Among 5,492 patients undergoing VA-ECMO (mean age 54.7 ± 15.1 years, 3,917 [71.3%] male), 832 (15.1%) received IABP after VA-ECMO. Before VA-ECMO, a higher incidence of cardiac intervention (13.9% vs. 16.7%) and myocardial infarction (12.0% vs. 14.8%) (all P < 0.05) was seen in the IABP after VA-ECMO group. In this cohort, the IABP after VA-ECMO group had a lower in-hospital mortality (52.5% vs. 48.0%, P = 0.017) and a higher survival rate on VA-ECMO (75.4% vs. 79.4%, P = 0.014). On multivariate modeling, the use of IABP after VA-ECMO was associated with a lower risk of in-hospital mortality (adjusted odds ratio[aOR], 0.823 [95% confidence interval [CI], 0.686–0.987]; P = 0.035) and on-support mortality (aOR, 0.828 [95% CI, 0.688–0.995]; P = 0.044). However, the use of IABP after VA-ECMO was also associated with an increased incidence of complications, including mechanical (aOR: 1.905, [95% CI, 1.278–2.839]; P = 0.002), bleeding (aOR: 1.371, [95% CI, 1.092–1.721]; P = 0.007), renal (aOR: 1.252, [95% CI, 1.041–1.505]; P = 0.017), and pulmonary (aOR: 1.768, [95% CI, 1.446–2.163]; P < 0.001).在5492例接受VA-ECMO的患者中(平均年龄54.7±15.1岁,3917例[71.3%]为男性),832例(15.1%)在VA-ECMO后接受了IABP。在VA-ECMO之前,IABP后VA-ECMO组的心脏干预(13.9%对16.7%)和心肌梗死(12.0%对14.8%)发生率更高(所有P<0.05)。在这组患者中,IABP后VA-ECMO组的住院死亡率较低(52.5%对48.0%,P=0.017),VA-ECMO存活率较高(75.4%对79.4%,P=0.014)。在多变量模型中,VA-ECMO后使用IABP与较低的住院死亡率风险相关(调整后的比值比[aOR],0.823[95%置信区间[CI],0.686-0.987];P=0.035),以及在支持下的死亡率(aOR,0.828[95% CI,0.688-0.995];P=0.044)。然而,VA-ECMO后使用IABP也与并发症发生率增加相关,包括机械性(aOR:1.905,[95% CI,1.278-2.839];P=0.002)、出血(aOR:1.371,[95% CI,1.092-1.721];P=0.007)、肾脏(aOR:1.252,[95% CI,1.041-1.505];P=0.017)和肺部(aOR:1.768,[95% CI,1.446-2.163];P<0.001)。
Conclusion
In this multicenter retrospective study, the use of IABP after VA-ECMO was associated with lower in-hospital mortality in patients with CS. These findings suggest that IABP may offer advantages for LV unloading in patients with CS treated with VA-ECMO, but further validation through randomized controlled trials is warranted to better understand the balance of risks and benefits.在这项多中心回顾性研究中,VA-ECMO后使用IABP与CS患者的住院死亡率降低相关。这些发现表明,IABP可能为接受VA-ECMO治疗的CS患者提供LV减负荷的优势,但需要通过随机对照试验进一步验证,以更好地理解风险和效益的平衡。
原创文章(本站视频密码:66668888),作者:xujunzju,如若转载,请注明出处:https://zyicu.cn/?p=19453
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫