Abstract
Importance: Prompt antimicrobial therapy is essential in sepsis, but accelerating antimicrobial administration may increase overtreatment.
重要性:及时使用抗菌药物治疗脓毒症至关重要,但加快抗菌药物的使用可能会增加过度治疗的风险。
Objectives: To examine the extent of and factors associated with physician variation in time from emergency department (ED) presentation to antimicrobial administration (hereinafter termed door-to-antimicrobial time) for sepsis and to assess whether faster practice patterns are associated with overtreatment.
目的:探讨急诊科(ED)就诊到给予抗菌药物时间(以下简称“门到抗菌药物时间”)在脓毒症患者中存在的医生间差异程度及其相关因素,并评估更快的治疗模式是否与过度治疗相关。
Design, setting, and participants: This explanatory mixed-methods study linked a quantitative retrospective cohort (July 1, 2013, to January 31, 2017) involving 30-day patient follow-up with prospective qualitative physician interview data (May 17, 2022, to June 28, 2023) at 4 Utah EDs. Participants included ED attending physicians and their patients meeting sepsis criteria (including intravenous antimicrobial administration) before ED departure. Data analysis occurred from 2021 to 2025.
设计、场所与参与者:本解释性混合方法研究将一项定量回顾性队列研究(2013年7月1日至2017年1月31日,含30天患者随访)与前瞻性定性医生访谈数据(2022年5月17日至2023年6月28日)相结合,研究对象来自犹他州的4家急诊科。参与者包括急诊主治医生及其在离开急诊科前符合脓毒症标准(包括静脉给予抗菌药物)的患者。数据分析时间为2021年至2025年。
Main outcomes and measures: Assessment for physician door-to-antimicrobial time variation used a likelihood ratio test comparing a linear mixed-effects model incorporating physician-level random intercepts and patient-level covariates with a model without physician random effects. Empirical best linear unbiased predictions of the physician random intercepts (termed physician-predicted mean door-to-antimicrobial times) quantified variation. The primary analysis used a joint mixed-effects shared parameter model to evaluate the association of physicians’ door-to-antimicrobial practice patterns with their overtreatment rate (infection ruled out on final retrospective adjudication). Qualitative analysis of semistructured cognitive task analysis interviews compared ED physicians in the fastest and slowest door-to-antimicrobial time quartiles.
主要结局与测量指标:评估医生之间门到抗菌药物时间的差异时,采用似然比检验比较包含医生层面随机截距与患者层面协变量的线性混合效应模型与不纳入医生随机效应的模型。通过经验最佳线性无偏预测(称为医生预测的平均门到抗菌药物时间)量化差异。主要分析采用联合混合效应共享参数模型,评估医生的门到抗菌药物实践模式与其过度治疗率(最终回顾性裁定排除感染者)之间的关系。对半结构化认知任务分析访谈进行定性分析,比较门到抗菌药物时间最快和最慢四分位数内的急诊科医生。
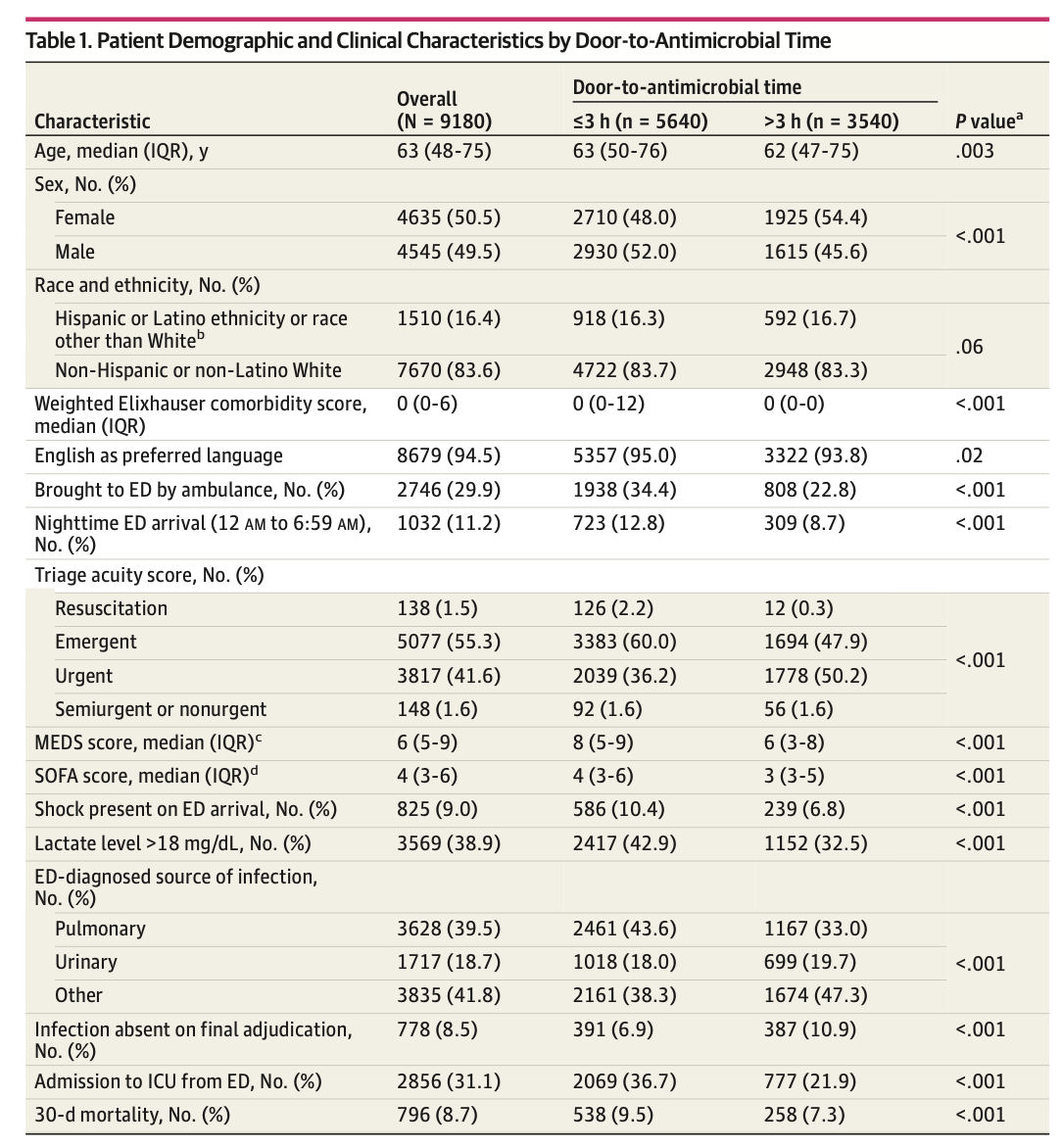
Results: Quantitative analyses included 88 ED physicians (71 [80.7%] male; median age, 39 [IQR, 35-49] years) and 9810 patients with sepsis (median age, 63 [IQR, 48-75] years), of whom 4635 (50.5%) were female and 3540 (38.6%) received antimicrobials more than 3 hours after ED arrival. The median number of patient encounters per physician was 105 (IQR, 75-129). Physicians’ door-to-antimicrobial time varied significantly (likehood ratio test P < .001), with average physician-level estimated mean door-to-antimicrobial time of 184 (95% estimation interval, 146-222) minutes for a typical patient, but was not associated with overtreatment (adjusted odds ratio, 0.98 [95% CI 0.94-1.02] per 10-minute increase in physician estimated mean door-to-antimicrobial time; P = .37). Among 18 physicians interviewed, physicians with faster door-to-antimicrobial times emphasized proactive, parallel task execution and care team coordination, while physicians with slower times described a more reactive and stepwise sepsis evaluation and treatment process.
结果:定量分析纳入88名急诊科医生(男性71人[80.7%],中位年龄39岁[IQR,35–49岁])及9810例脓毒症患者(中位年龄63岁[IQR,48–75岁]),其中女性4635人(50.5%),3540人(38.6%)在到达急诊科后超过3小时才接受抗菌药物治疗。每位医生接诊患者的数量中位数为105例(IQR,75–129)。医生之间的门到抗菌药物时间存在显著差异(似然比检验P < .001),典型患者的平均医生层面估计门到抗菌药物时间为184分钟(95%估计区间,146–222分钟),但与过度治疗无关(医生估计的平均门到抗菌药物时间每增加10分钟的调整比值比为0.98 [95%置信区间0.94–1.02];P = .37)。在接受访谈的18名医生中,门到抗菌药物时间较短的医生强调主动、并行执行任务和护理团队协作,而时间较长者则描述了一种更为被动、逐步进行的脓毒症评估与治疗流程。
Conclusions and relevance: In this mixed-methods study, ED physicians’ antimicrobial administration time for sepsis varied significantly, but faster antimicrobial initiation practice patterns were not associated with overtreatment. Physicians with shorter door-to-antimicrobial times described a proactive, parallel processing approach to sepsis care.
结论与相关性:在这项混合方法研究中,急诊科医生在脓毒症抗菌药物治疗时间上存在显著差异,但较快的抗菌药物启动模式并未与过度治疗相关。门到抗菌药物时间较短的医生描述了一种积极主动、并行处理的脓毒症护理方式。
原创文章(本站视频密码:66668888),作者:xujunzju,如若转载,请注明出处:https://zyicu.cn/?p=21616
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫