Abstract
Objectives: Venoarterial extracorporeal membrane oxygenation (ECMO) is associated with neurologic complications but their impact on long-term outcomes are poorly understood. Our objective was to assess the association of neurologic complications with death and new disability at 6 months.
目的:静脉‑动脉体外膜肺氧合(ECMO)与神经系统并发症相关,但这些并发症对长期结局的影响尚不清楚。本研究旨在评估神经系统并发症与6个月时死亡及新发残疾之间的关联。
Design: Prospective, multicenter, observational study.
设计:前瞻性、多中心、观察性研究。
Setting: Thirty ECMO centers in Australia and New Zealand between February 2019 and December 2022.
地点:2019年2月至2022年12月期间,澳大利亚和新西兰的30家ECMO中心。
Subjects: seven hundred four adult patients admitted to the ICU on venoarterial ECMO other than for extracorporeal cardiopulmonary resuscitation.
研究对象:704名因非体外心肺复苏而入住ICU并接受静脉‑动脉ECMO治疗的成年患者。
Interventions: None.
干预措施:无。
Measurement and main results: Patients were divided according to whether they experienced neurologic complications. Neurologic complications include diffuse cerebral ischemia, stroke, cerebral hemorrhage, and brain death. The primary outcome was a composite of death or new disability at 6 months. Secondary outcomes included disability measured by the World Health Organization Disability Assessment Schedule and quality of life measured with EuroQoL 5D five levels. The median age of patients was 54.5 years (42-64 yr) and 259 (36.8%) were female. The primary outcome was available for 613 of 706 patients (86.2%). Of these, 425 patients (69.3%) had either died or had new disability at 6 months. Neurologic events occurred in 85 patients (12%). Patients who experienced neurologic complications were at increased risk of death or new disability (risk difference [RD], 17.28% [6.44-25.92%]). This was primarily due to an increased risk of mortality RD, 23.75 (12.06-34.75) rather than new disability (RD, -11.90% [-30.58% to 13.56%]). These findings were consistent across types of complications and after adjustment for confounders. Patients with neurologic complications more commonly had ECMO discontinued due to a perceived poor prognosis (odds ratio, 2.7; 95% CI, 1.35-24.7).
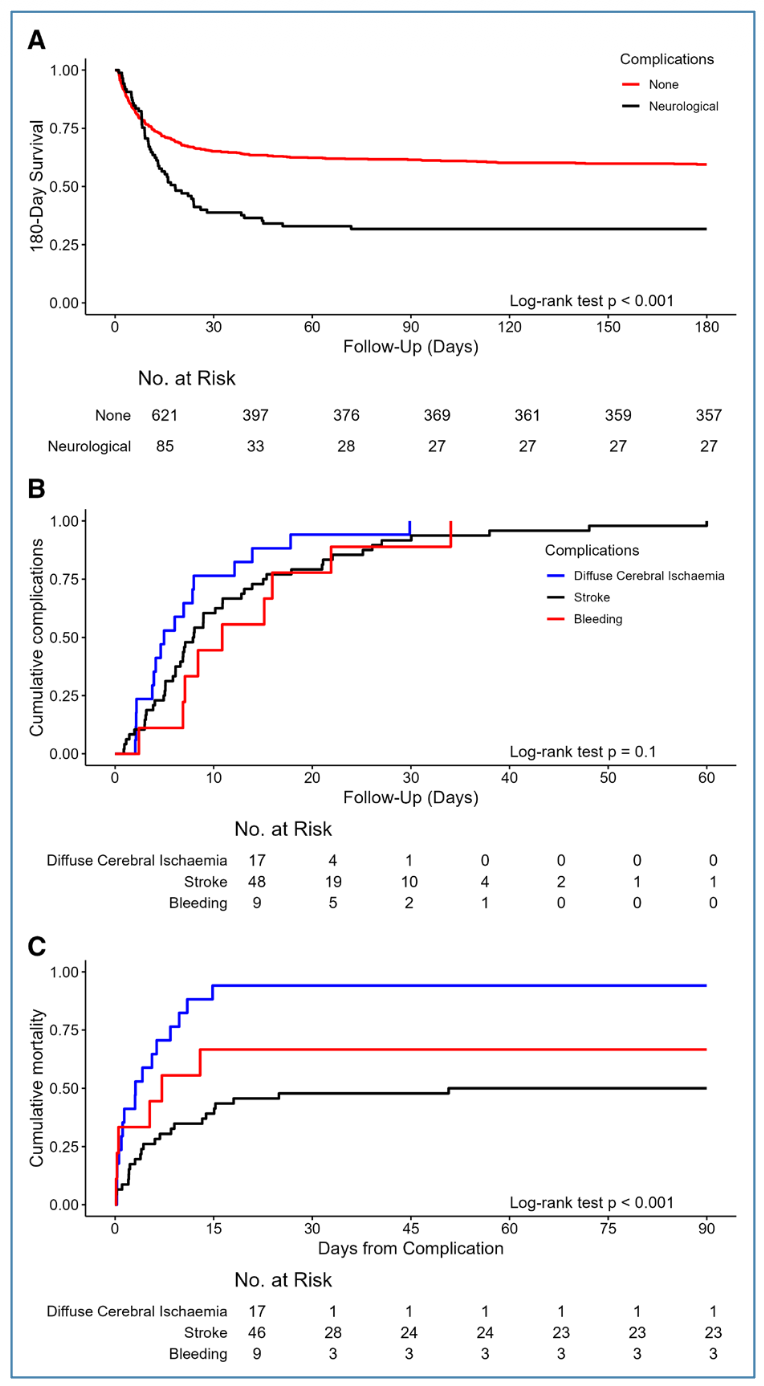
测量指标与主要结果:根据患者是否发生神经系统并发症进行分组。神经系统并发症包括弥漫性脑缺血、脑卒中、脑出血和脑死亡。主要结局为6个月时的死亡或新发残疾的复合事件。次要结局包括采用世界卫生组织残疾评估量表(WHODAS)测量的残疾情况,以及采用欧洲五维健康量表五水平版(EuroQoL 5D‑5L)测量的生活质量。患者的中位年龄为54.5岁(42–64岁),其中女性259人(36.8%)。706名患者中有613人(86.2%)可获得主要结局数据。在这些患者中,425人(69.3%)在6个月时死亡或伴有新发残疾。85名患者(12%)发生了神经系统事件。经历神经系统并发症的患者死亡或新发残疾的风险增加(风险差[RD] 17.28% [6.44%–25.92%])。这主要是由于死亡风险增加(RD 23.75% [12.06%–34.75%]),而非新发残疾风险增加(RD –11.90% [–30.58% 至 13.56%])。在不同类型的并发症中以及调整混杂因素后,上述结果保持一致。神经系统并发症患者更常因被认为预后不良而中止ECMO(比值比 2.7;95% CI 1.35–24.7)。
Conclusions: Neurologic complications during ECMO increased the risk of death and disability at 6 months, primarily driven by increased death at 6 months. Prevention of these complications and development of better prognostic tools for functional outcomes should be prioritized.
结论:ECMO期间的神经系统并发症会增加6个月时的死亡和残疾风险,主要由死亡风险升高驱动。应优先致力于预防这些并发症的发生,并开发更好的功能结局预测工具。
原创文章(本站视频密码:66668888),作者:xujunzju,如若转载,请注明出处:https://zyicu.cn/?p=21309
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫