Abstract
Background: The optimal approach to early resuscitation in septic shock is unknown. Equipoise exists between the use of larger volumes of intravenous fluids to restore perfusion and the use of early vasopressor therapy along with smaller volumes of fluids to minimize potential harm from excess fluid.感染性休克早期复苏的最优方案尚无定论。目前存在两种平衡争议方案:一是输注大剂量静脉液体以恢复组织灌注;二是早期启用血管活性药物、同时限制液体入量,减少液体过量带来的潜在损伤。
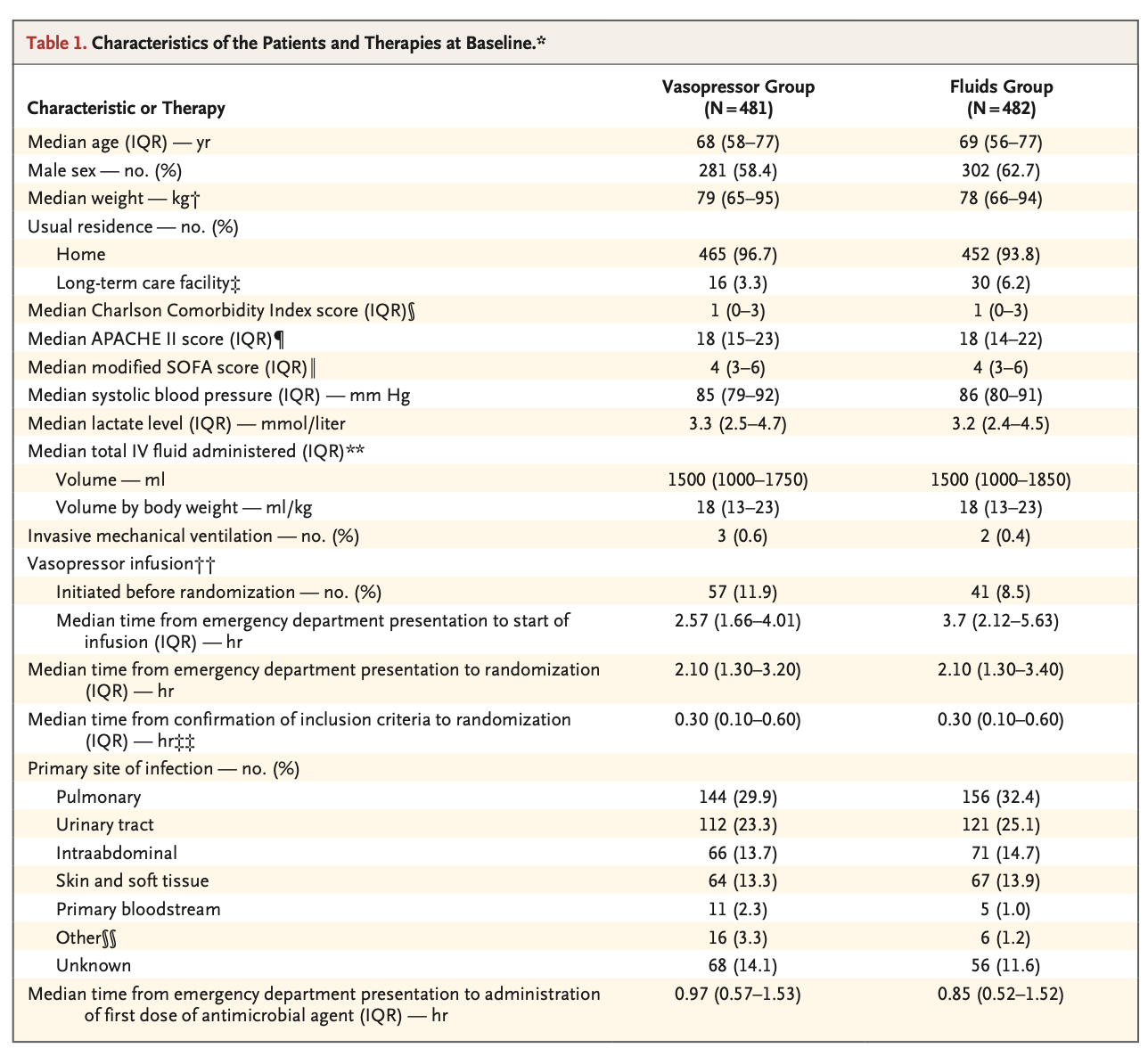
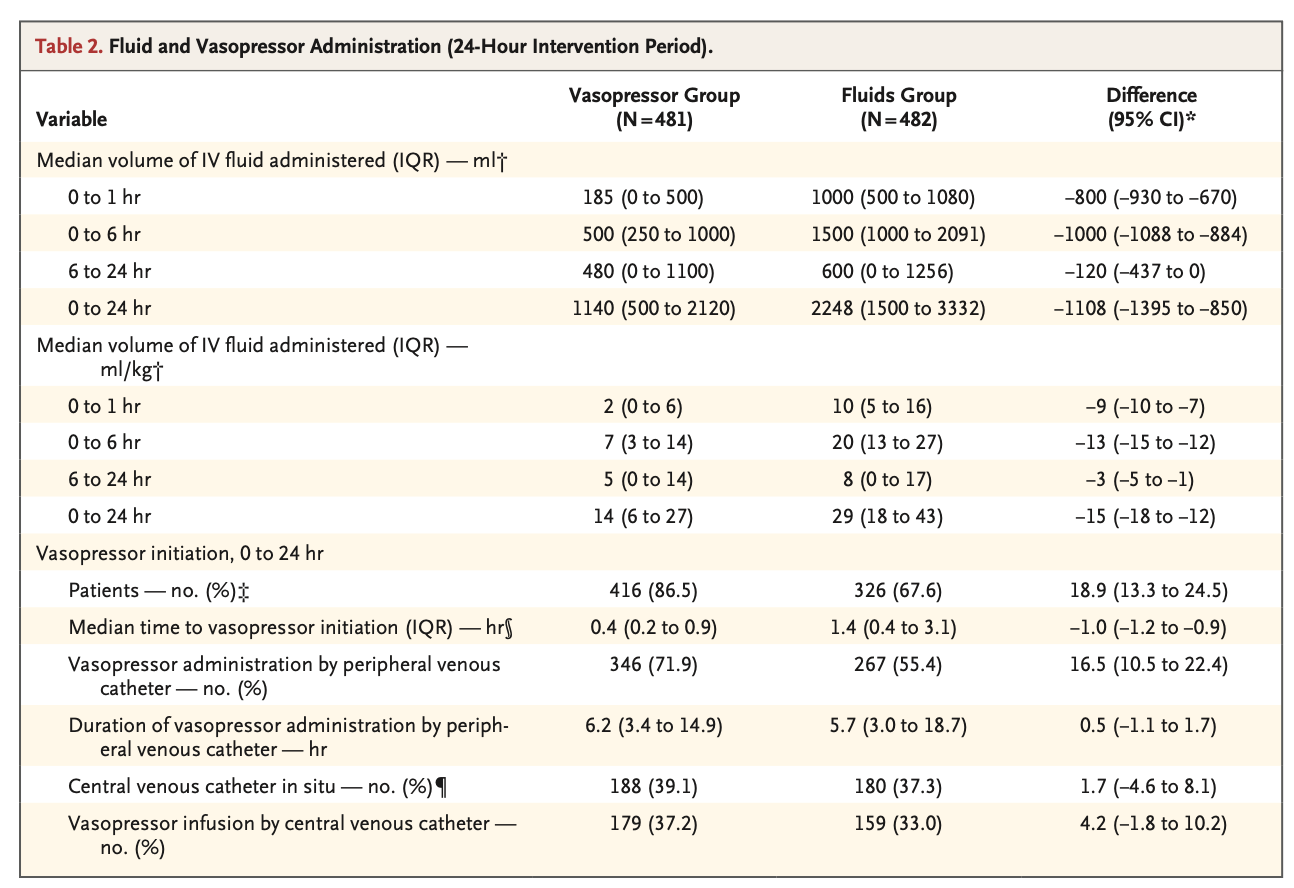
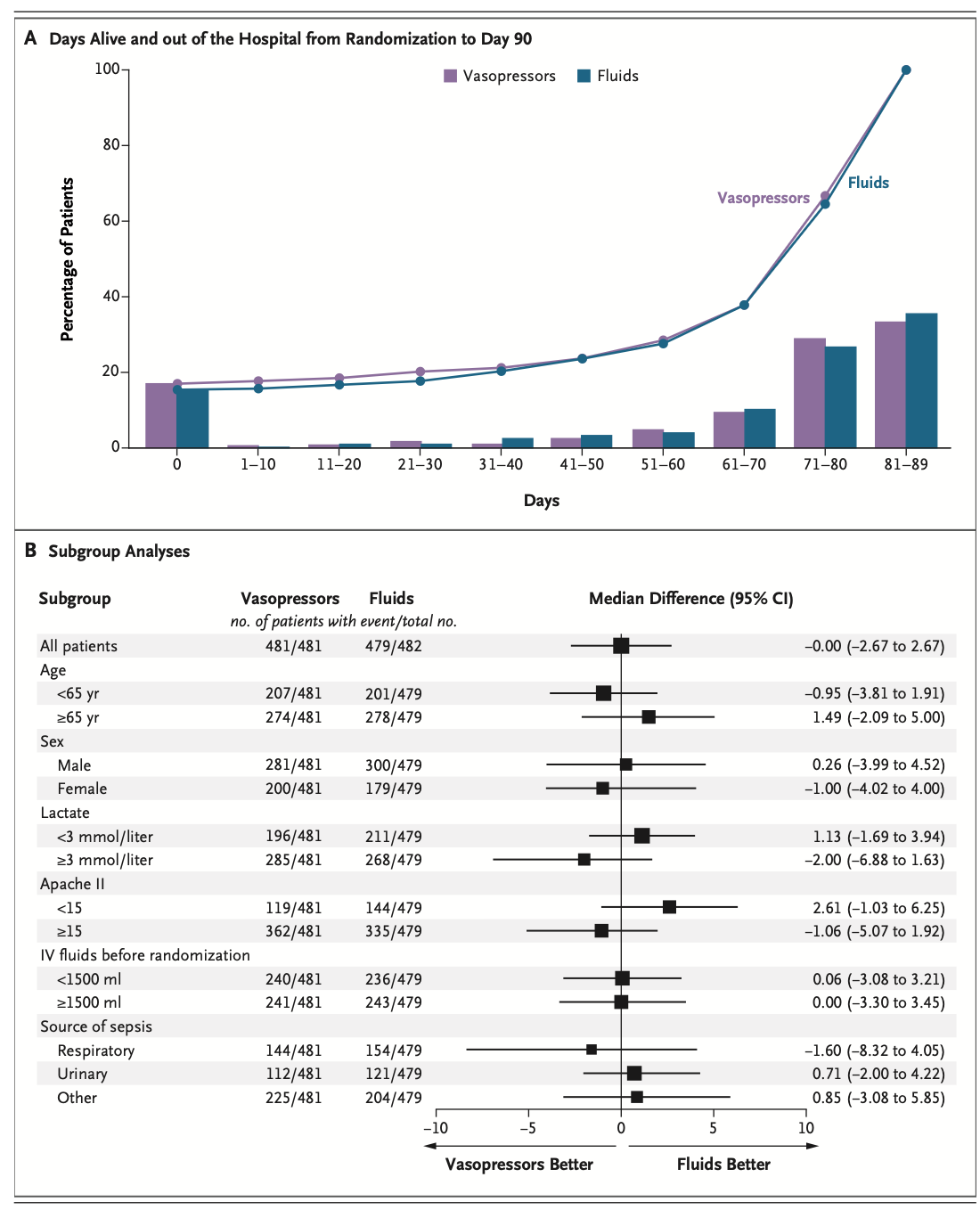
Methods: We randomly assigned adult patients who presented to the emergency department with septic shock to receive either fluids at restricted volumes and early vasopressor therapy (vasopressor group) or higher volumes of fluids and later vasopressor therapy (fluids group) for at least 6 hours and up to 24 hours. The primary outcome was days alive and out of the hospital from randomization to day 90.本研究将急诊科就诊的成人感染性休克患者随机分为两组:限制液体 + 早期血管活性药物组(血管活性药物组)、足量液体 + 延迟血管活性药物组(液体组),干预持续至少 6 小时、最长 24 小时。主要终点为随机分组后至第 90 天,患者存活且脱离住院的总天数。
Results: A total of 1000 patients underwent randomization, with 499 assigned to the vasopressor group and 501 to the fluids group. Informed consent was not obtained for 37 patients, which left 963 patients in the intention-to-treat population (481 in the vasopressor group and 482 in the fluids group). Three patients in the fluids group were lost to follow-up for the primary outcome. In the first 24 hours after randomization, patients in the vasopressor group received less intravenous fluid than those in the fluids group (median difference, -1108 ml; 95% confidence interval [CI], -1395 to -850). The percentage of patients who received vasopressors was higher by 18.9 percentage points (95% CI, 13.3 to 24.5) in the vasopressor group. The median number of days alive and out of the hospital at day 90 was 76 (interquartile range, 55 to 83) in the vasopressor group and 76 (interquartile range, 55 to 82) in the fluids group (difference, 0.0 days; 95% CI, -2.7 to 2.7; P = 1.00). Adverse events occurred in similar percentages of patients in the two groups, except for pulmonary edema (0.6% in the vasopressor group vs. 5.0% in the fluids group; P<0.001).本研究共纳入 1000 例患者完成随机分组,血管活性药物组 499 例,液体组 501 例。其中 37 例未获取知情同意,意向治疗人群最终为 963 例(血管活性药物组 481 例,液体组 482 例);液体组 3 例患者主要终点失访。随机分组后 24 小时内,血管活性药物组静脉液体输注量显著少于液体组(中位数差值 – 1108 毫升,95% 置信区间 – 1395 ~ -850);血管活性药物使用率较液体组高出 18.9 个百分点(95% 置信区间 13.3 ~ 24.5)。第 90 天时,血管活性药物组患者存活且出院天数中位数为 76 天(四分位距 55~83),液体组同样为 76 天(四分位距 55~82),组间差值 0 天(95% 置信区间 – 2.7 ~ 2.7,P=1.00)。两组总体不良事件发生率相近,仅肺水肿发生率存在显著差异:血管活性药物组 0.6%,液体组 5.0%(P<0.001)。
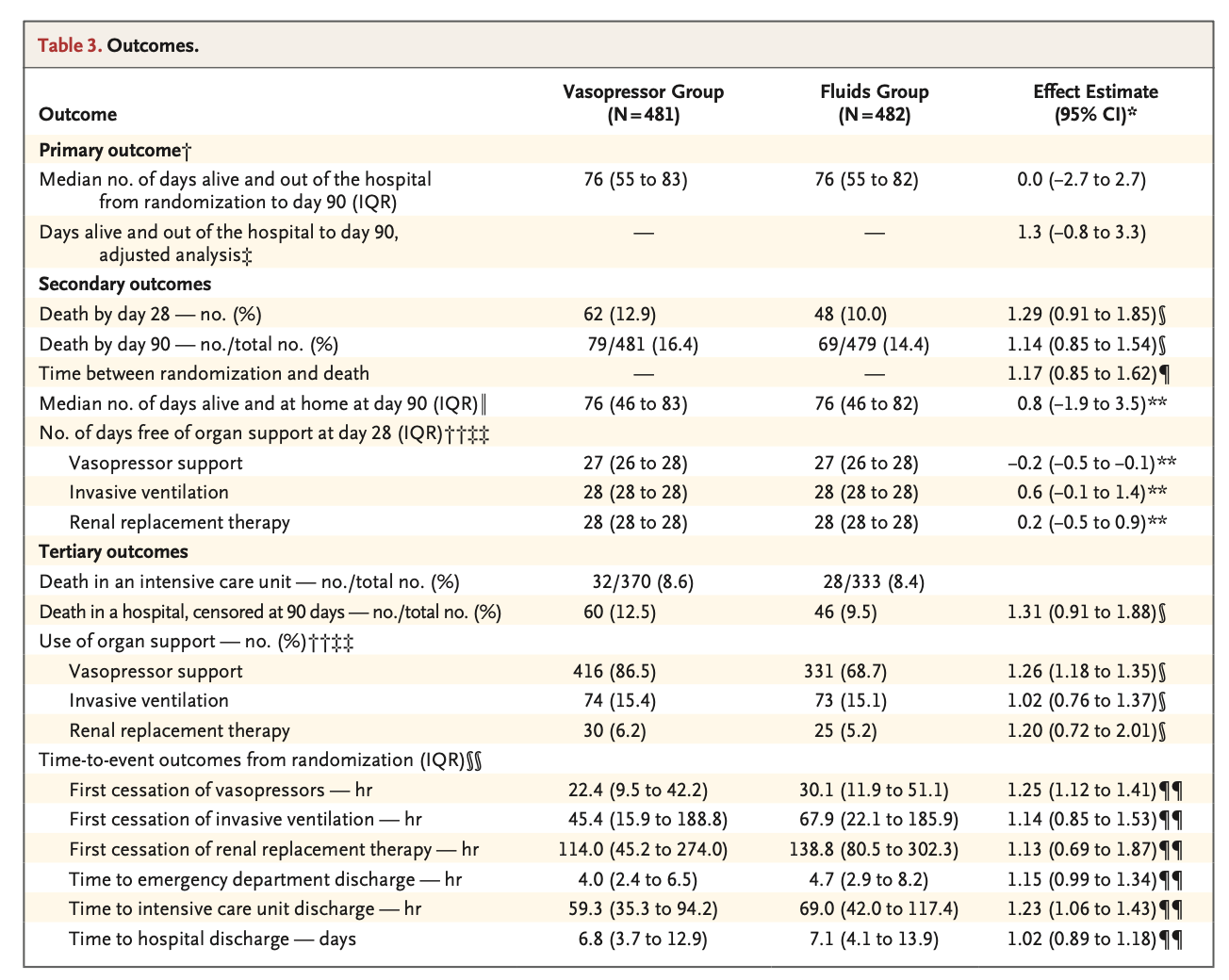
Conclusions: Among adult patients who presented to the emergency department with septic shock, an approach that involved restricted fluid volume and early vasopressors did not result in a greater number of days alive and out of the hospital at day 90 than an approach involving greater fluid volume and later administration of vasopressors. 针对急诊科就诊的成人感染性休克患者,限制液体输注联合早期使用血管活性药物的复苏策略,与大量液体复苏、延迟启用血管活性药物相比,并未提升患者 90 天内存活且脱离住院的总天数。
所以是不是可以早点用去加了?
原创文章(本站视频密码:66668888),作者:xujunzju,如若转载,请注明出处:https://zyicu.cn/?p=22101
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫