Abstract
Background
Liver abscess (LA) is a rare but potentially serious condition with a high mortality rate. Current epidemiological data of LA patients requiring intensive care unit (ICU) admission are limited.
肝脓肿(LA)是一种罕见但可能危及生命的疾病,死亡率较高。目前关于需要入住重症监护病房(ICU)的肝脓肿患者的流行病学数据十分有限。
Methods
This multicentre retrospective study included adults admitted to 24 ICUs in France between January 2010 and December 2020. Risk factors for mortality were identified by multivariate analysis. A propensity score was used to adjust for confounders related to the presence of portal vein thrombosis.
这项多中心回顾性研究纳入了2010年1月至2020年12月期间入住法国24个ICU的成年患者。通过多变量分析确定死亡的危险因素。使用倾向评分来调整与门静脉血栓形成相关的混杂因素。
Results
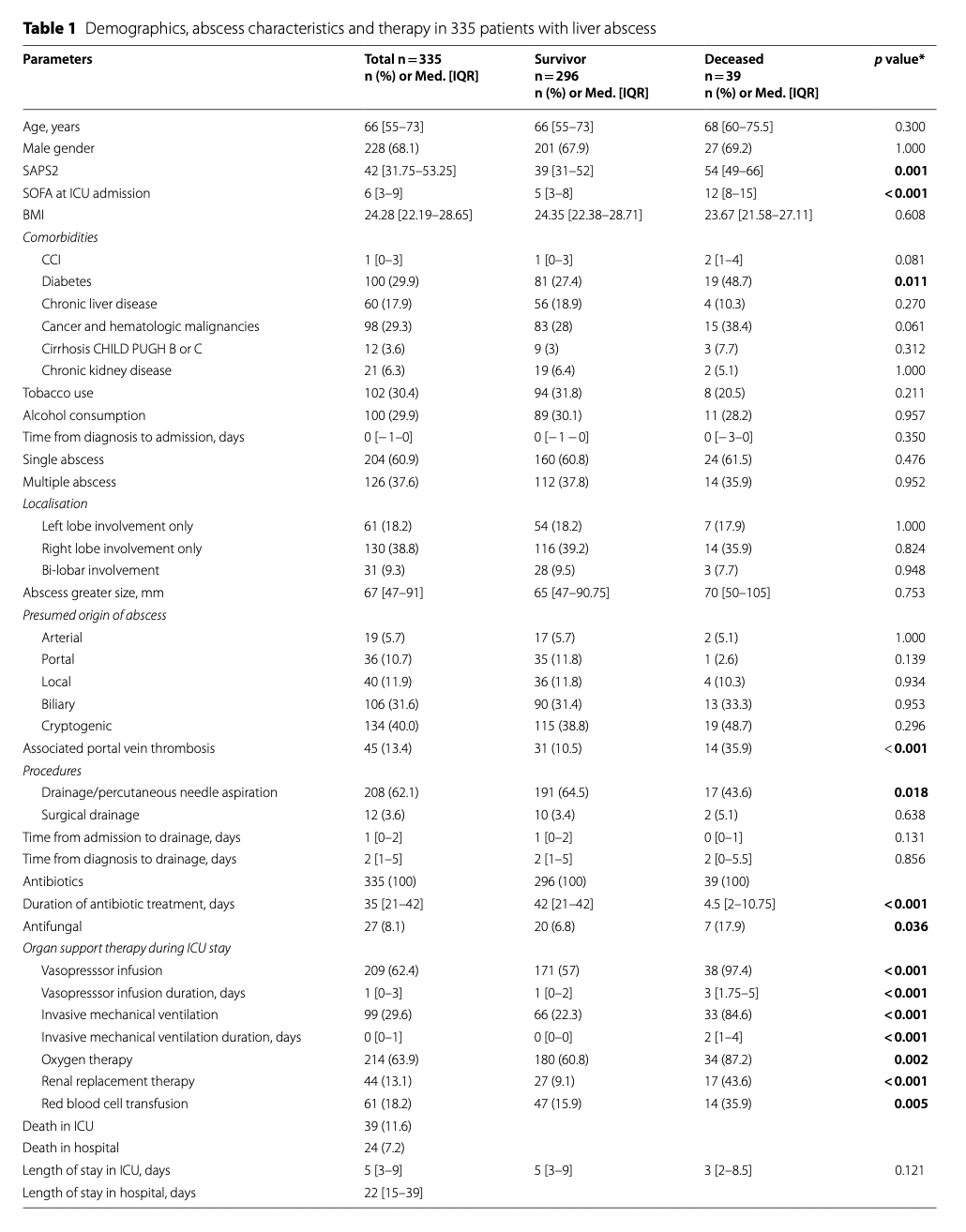
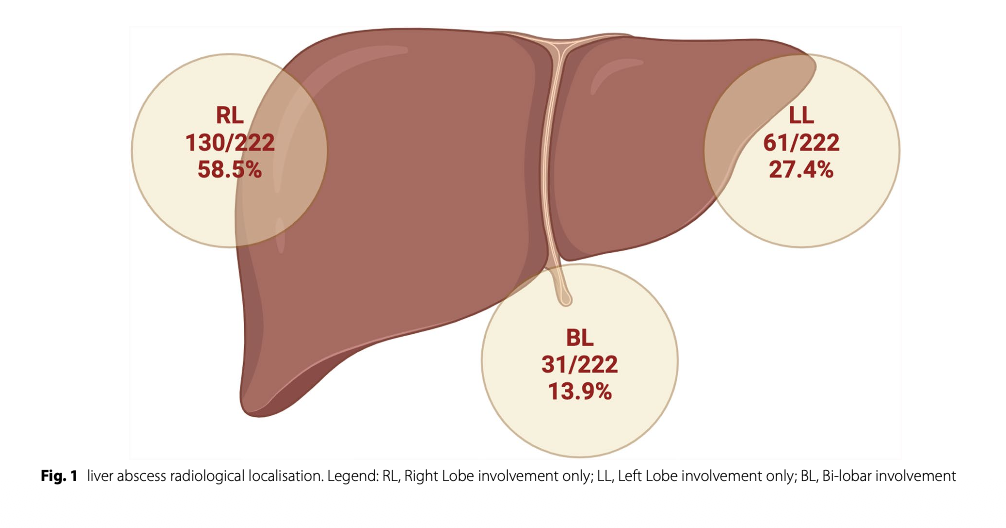
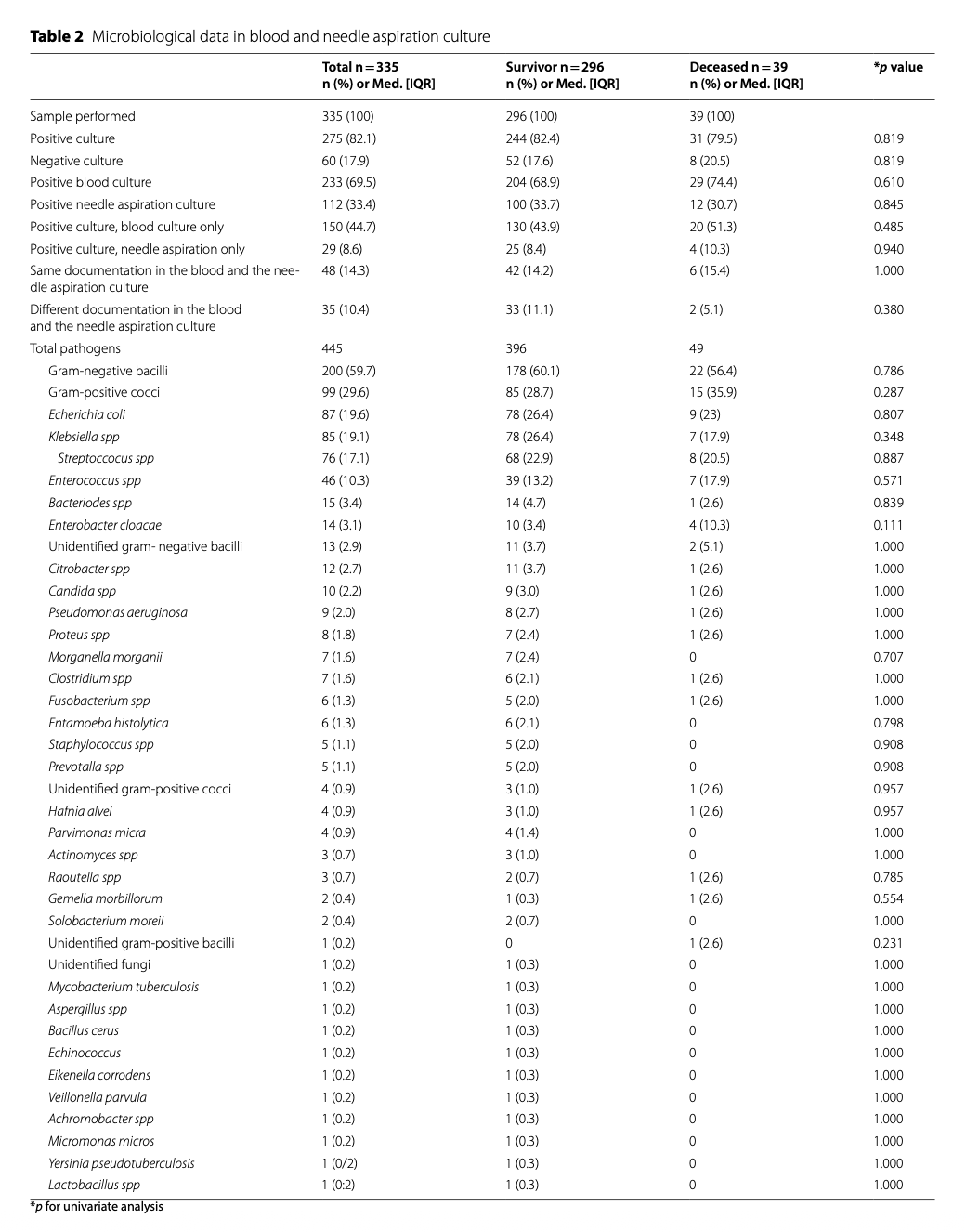
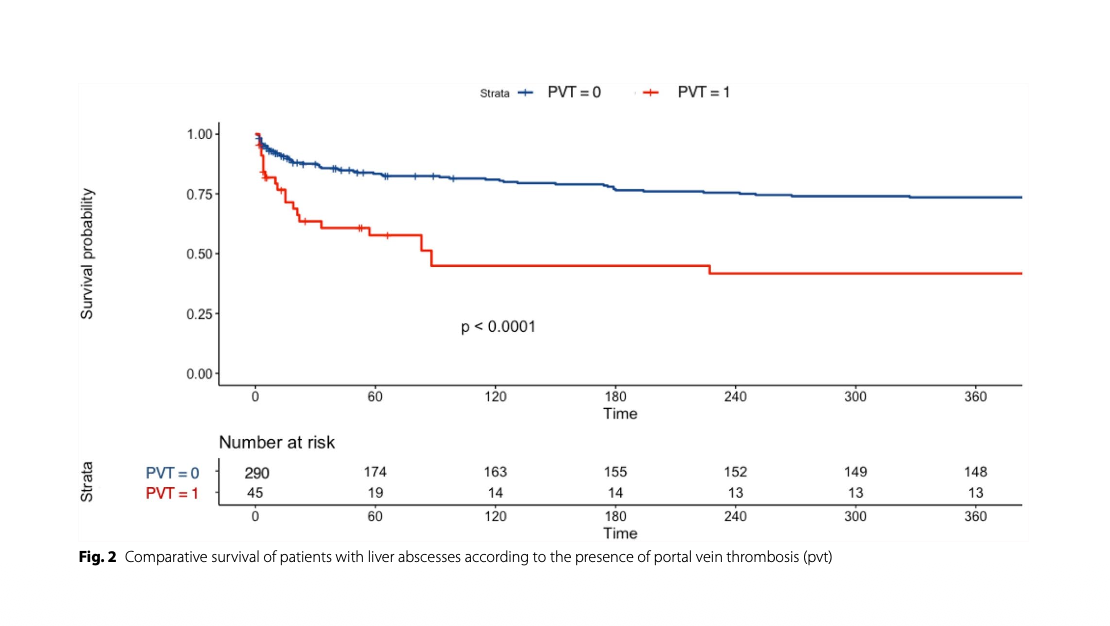
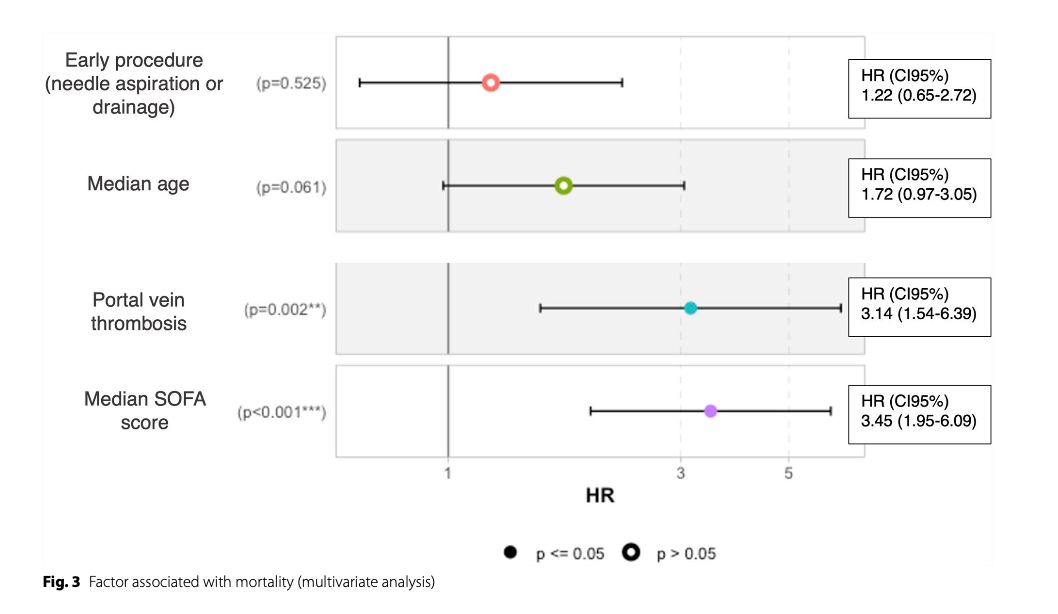
335 patients were enrolled. The median age was 66 years [53–73] and 68% were male. Commons comorbidities included diabetes (29.9%) and cancer or haematological disease. Septic shock was the main reason for admission (58%). The median SAPS2 score at ICU admission was 42 [31–53] and the SOFA score was 6 [3–9]. The putative origin of LA was biliary (31%), while 40% were cryptogenic. Most patients (60%) had a solitary LA, involving the right lobe (38.8%), with a median diameter of 67 mm [47–91]. Associated portal vein thrombosis (PVT) was present in 13.4% of cases. Microbiological documentation was obtained in 82% of patients, showing gram-negative bacilli (59.7%), mainly Escherichia coli (19.6%) and Klebsiella spp. (19.1%), and gram-positive cocci (29.6%), mainly Streptococcus spp. (17.1%). Drainage was performed in 62% of cases, 40% within 48 h. The median duration of antibiotic therapy was 35 days [21–42]. During hospitalisation, 62% of patients required vasopressors and 29% required mechanical ventilation. In-ICU mortality was 11.6%. Multivariate analysis showed that organ dysfunction illustrated by SOFA score (HR 3.45 [1.95–6.09], p < 0.001) and PVT (HR 3.14 [1.54–6.39], p = 0.001) were significant risk factors for mortality. Drainage was not associated with improved short-term survival (HR 1.22 [0.65–2.72], p = 0.52). In the population matched for PVT confounders, a higher sofa score was the only factor associated with mortality (HR 3.11 [1.76–5.49] IC95%, p = 0.001).
共纳入335名患者。中位年龄为66岁[53–73],男性占68%。常见合并症包括糖尿病(29.9%)以及癌症或血液系统疾病。感染性休克是主要的入院原因(58%)。入ICU时的中位SAPS2评分为42分[31–53],SOFA评分为6分[3–9]。肝脓肿的推测来源为胆道源性(31%),而40%为隐源性。大多数患者(60%)为单发脓肿,累及右叶(38.8%),中位直径为67毫米[47–91]。13.4%的病例伴有门静脉血栓(PVT)。82%的患者获得了微生物学证据,显示主要为革兰氏阴性杆菌(59.7%),其中大肠杆菌(19.6%)和克雷伯菌属(19.1%)最为常见;以及革兰氏阳性球菌(29.6%),主要是链球菌属(17.1%)。62%的患者接受了引流治疗,其中40%在48小时内进行。抗生素治疗的持续时间为35天[21–42]。住院期间,62%的患者需要使用血管加压药,29%需要机械通气。ICU内死亡率为11.6%。多变量分析显示,以SOFA评分衡量的器官功能障碍(HR 3.45 [1.95–6.09], p < 0.001)和门静脉血栓(HR 3.14 [1.54–6.39], p = 0.001)是死亡的显著危险因素。引流治疗与短期生存率改善无关(HR 1.22 [0.65–2.72], p = 0.52)。在针对PVT混杂因素匹配的人群中,较高的SOFA评分是唯一与死亡率相关的因素(HR 3.11 [1.76–5.49] 95%CI, p = 0.001)。
Conclusions
This multicentre study illustrates the severity of LA in French intensive care units and identifies organ dysfunction (SOFA score) and portal vein thrombosis as major risk factors for mortality. Prospective studies are needed to improve management strategies, as the survival benefit of drainage is unclear.
这项多中心研究说明了肝脓肿在法国重症监护病房中的严重性,并确定器官功能障碍(SOFA评分)和门静脉血栓形成是主要的死亡危险因素。由于引流治疗的生存获益尚不明确,需要进行前瞻性研究以改进管理策略。
原创文章(本站视频密码:66668888),作者:xujunzju,如若转载,请注明出处:https://zyicu.cn/?p=21774
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫