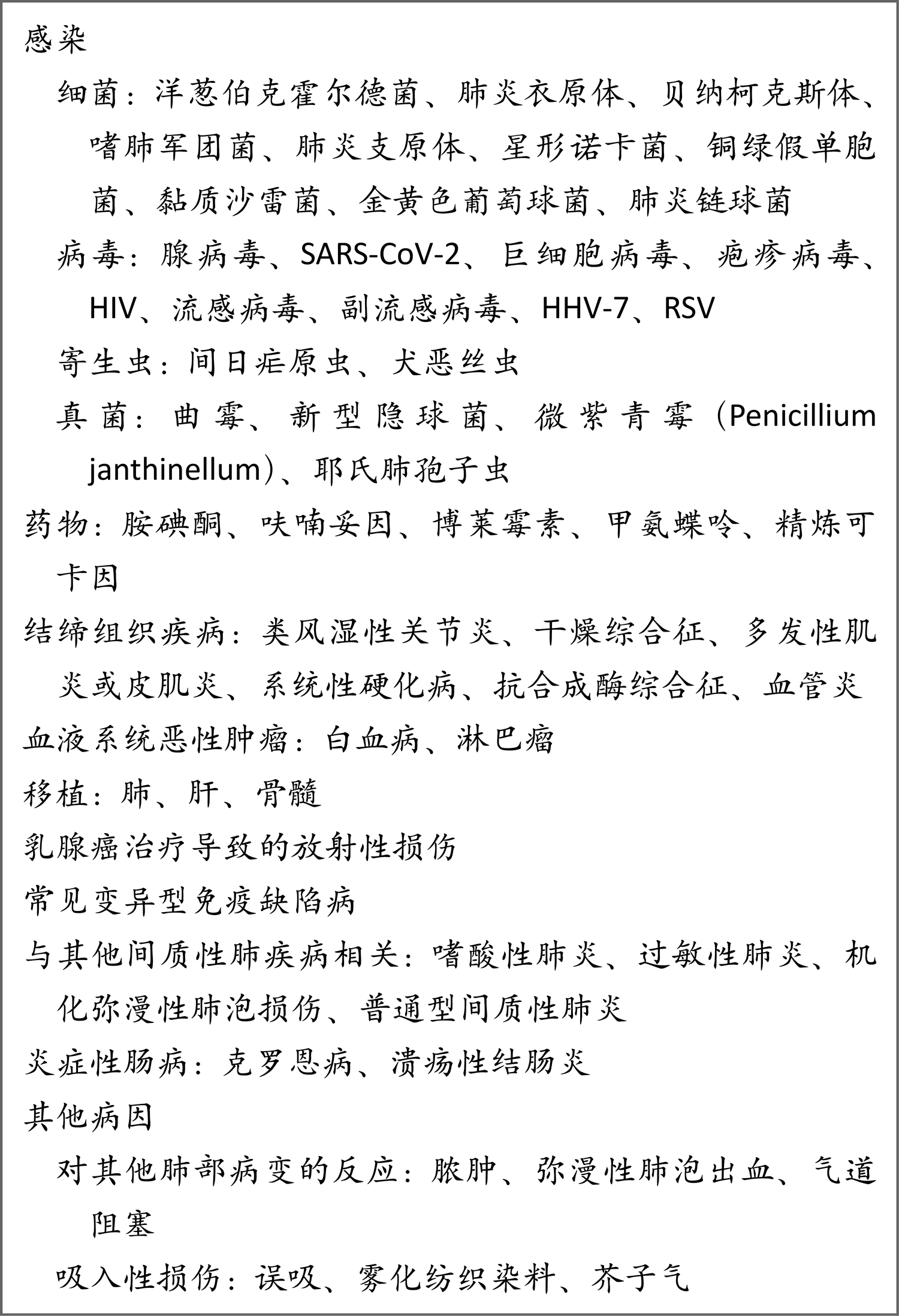
机化性肺炎是肺损伤后的肺组织修复模式。它可以是隐源性,也可以是对特定肺损伤的应答,在组织病理学水平也可见于多种不同临床背景。隐源性机化性肺炎(COP)无明确病因,被归类为特发性间质性肺炎1-4。这类肺炎以前称为闭塞性细支气管炎伴机化性肺炎,它在临床上受到关注,原因是常被误诊,并且治疗得当的情况下康复率高。继发性机化性肺炎可归因于特定原因(如病毒感染、药物毒性、吸入性损伤、放疗或癌症),或者与明确临床背景相关(如结缔组织疾病、误吸、移植后遗症或其他间质性肺炎)5(表1)。
流行病学
COP在世界各地均有报道,但确切发病率和患病率尚不清楚。与以前的病例系列研究相比6,13,最近的报道指出COP诊断率较低14,15,原因可能是我们对继发性机化性肺炎的病因逐渐了解5。冰岛一项全国性回顾性研究表明,在20年期间,COP的年平均发病率为每10万人中1.10例16。据报道,在加拿大一家大型教学医院,累积患病率为每10万例住院患者中6.7例13。在关于间质性肺疾病的登记系统研究中,该人群的COP患病率在一项研究中为5%,在另一项研究中为10% 18。
根据世界各地治疗中心发表的37份报道(共1,490例COP确诊患者),患者确诊时的平均年龄为50~60岁(范围,17~95岁);儿童中很少有关于COP的报道1,6-11,14,19-47。男性发病率略高于女性(男性发病率为52%)。约54%的COP患者从未吸烟,46%既往或当前吸烟;在既往或当前吸烟者中,确诊时有不到15%的人自诉当前吸烟。有人提出,环境因素在COP发生中起一定作用14,48。
病理生理学
机化性肺炎的发病机制尚不清楚2,3,5。肺损伤似乎发生于某一时刻,并且未严重破坏肺结构。COP是炎性和纤维增生过程,以肺泡内纤维增生为特征,经过免疫抑制或抗炎治疗后可逆(有时不可逆)。这一模式与其他纤维化过程形成鲜明对比,特别是普通型间质性肺炎(UIP),UIP不可逆2,3(图1)。
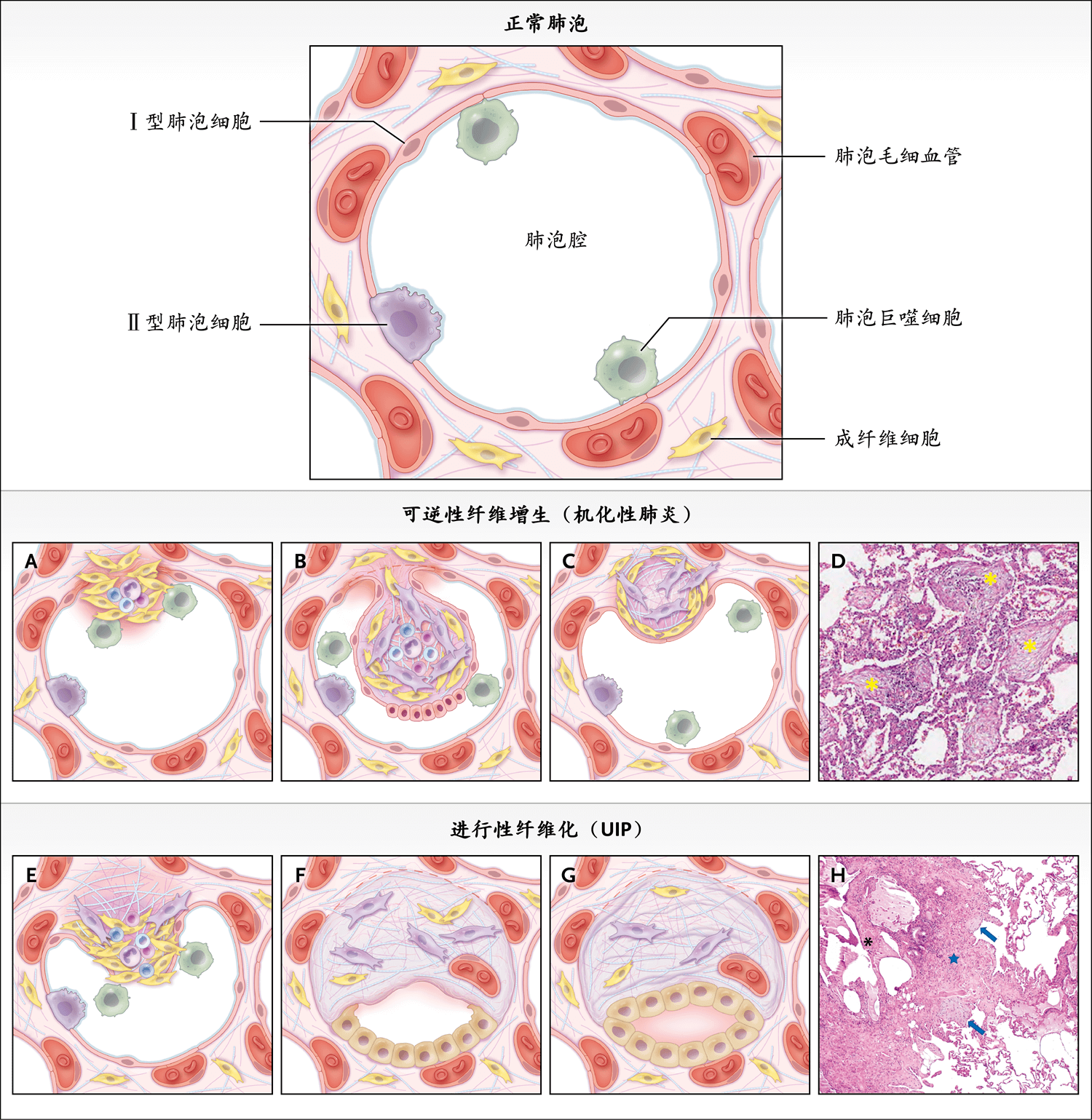
上图为正常肺泡。图A显示机化性肺炎的肺泡损伤。上皮细胞损伤伴上皮基底层剥蚀导致出现间隙,之后血浆蛋白渗漏,纤维蛋白形成,炎症细胞迁移至肺泡腔。图B显示肺泡机化。炎症细胞和纤维蛋白沉积物并未破坏肺泡腔,而是从肺泡芽(alveolar bud)中消失。肺泡腔内的成纤维细胞激活、增殖并通过基底层间隙迁移,这导致纤维炎性芽(fibroinflammatory bud,Masson小体)形成。在这些水肿的肺泡芽内,毛细血管、小成纤维细胞(黄色)和肌成纤维细胞(淡紫色)主要表达基质金属蛋白酶。图C显示重构。消退过程开始后,纤维炎性芽被肌成纤维细胞取代,肌成纤维细胞与胶原束层交替,呈同心环状排列。芽并入肺泡壁,胶原束(胶原球)被Ⅰ型肺泡上皮细胞覆盖。这些细胞增殖并恢复肺泡毛细血管膜的连续性和肺泡单位的完整性。图D(苏木精和伊红染色)显示高倍放大的机化性肺炎的组织学特征。可见几个疏松结缔组织息肉样腔内栓(星号)。肺泡壁出现轻度慢性炎症。图E显示UIP中肺泡损伤产生的影响。上皮细胞反复微损伤导致血管的蛋白质(如纤维蛋白原和纤连蛋白)渗透性增加,导致临时基质(伤口凝块)形成。随后,细支气管和肺泡上皮细胞迁移到肺泡腔内并增殖。图F显示肺泡机化的微环境。上皮细胞异常激活并产生多种生长因子和趋化因子,这些因子诱导驻留成纤维细胞和骨髓来源的成纤维细胞祖细胞(纤维细胞)迁移到发生微损伤的部位。此外,图G显示肺泡纤维化,成纤维细胞(黄色)向肌成纤维细胞(淡紫色)分化,这些肌成纤维细胞因抗凋亡而少量聚集并持续留在病灶内。在病灶中,肌成纤维细胞分泌过多的细胞外基质蛋白(主要是纤维胶原蛋白),并主要表达金属蛋白酶2组织抑制物。肺泡塌陷和异常的进行性肺重构导致不同大小的囊肿,囊肿周围出现纤维化伴增生性或细支气管型上皮(蜂窝状)。图H(苏木精和伊红染色)显示高倍放大的UIP组织学特征。疏松的机化结缔组织的成纤维灶(箭形)与明显的纤维化毗连,纤维化组织由致密胶原瘢痕与肺结构重构(星号)和囊性改变(蜂窝状)(黑色星号)组成。图的右上部分为正常肺。
肺泡损伤
机化性肺炎的早期事件包括上皮基底层局部剥蚀和Ⅰ型肺泡上皮细胞坏死,导致基底层出现间隙49,50。肺泡上皮损伤后,血浆蛋白渗漏,纤维蛋白形成,炎症细胞(巨噬细胞、淋巴细胞、中性粒细胞、部分嗜酸性粒细胞,偶尔浆细胞和肥大细胞)迁移至肺泡腔内50-52(图1A)。
肺泡机化
成纤维细胞被募集到肺泡腔,在肺泡腔增殖,分化成肌成纤维细胞,并形成纤维炎性芽(Masson小体),这是机化性肺炎的特征52(图1B)。纤维炎性芽与疏松的结缔组织基质交错,基质内富含胶原蛋白(尤其是胶原Ⅰ)、纤连蛋白、Ⅲ型前胶原蛋白、生腱蛋白C和蛋白聚糖53,54。蛋白调节异常(涉及血管内皮生长因子、碱性成纤维细胞生长因子和基质金属蛋白酶[MMP])发生;在机化性肺炎中,蛋白质调节异常与新形成的腔内纤维黏液结缔组织的血管生成活性相关57。
重构
炎症细胞和纤维蛋白沉积物开始从肺泡芽中消失,取而代之的是肌成纤维细胞,它们与胶原束层交替,呈同心环状排列;胶原束层由薄的Ⅰ型胶原纤维、更薄的Ⅲ型胶原纤维和前胶原纤维,以及纤连蛋白组成5,49。肺泡内芽重构成间质,胶原球形成54(图1C)。胶原球由密集排列的胶原原纤维和成纤维细胞或肌成纤维细胞与细胞质组成,细胞质中含有肌动蛋白样微丝和吞噬型胶原原纤维,并被Ⅰ型肺泡上皮细胞覆盖,上皮基底膜完好。肺泡上皮细胞增殖并恢复肺泡毛细血管膜的连续性。肺泡单元的完整性和功能得到恢复5,49。根据报道,少数患者出现机化性肺炎的纤维化模式,其特征是最初出现机化性肺炎,几个月后出现非特异性间质性肺炎58,59。肺实质重构的特征是整个肺泡壁有残留间质炎症和纤维化59,60。肺泡结构保留,蜂窝改变少见。此外,未能将肺泡内芽从气腔再吸收到间质,以及未能形成胶原球可能是瘢痕性机化性肺炎的原因(见下文讨论)43,61。
Masson小体与成纤维细胞灶的比较
机化性肺炎的几个病理特征使其有别于其他纤维化肺病程(如UIP)62。首先,UIP的病理模式代表了上皮驱动的疾病,与遗传和环境危险因素和衰老相关过程(包括成纤维细胞激活、异常上皮和肌成纤维细胞分化63、细胞外基质重构,以及最终的终末期纤维化)之间的复杂相互作用相关64。其次,出现基底膜间隙(决定肺泡内纤维化受累的关键事件)的肺泡上皮损伤在机化性肺炎中不太广泛,也不太严重49。
第三,机化性肺炎的康复与疏松结缔组织芽(包含炎症细胞和成纤维细胞)周围的再上皮化相关52,55。再生的Ⅱ型肺泡上皮细胞以有序方式分层,通常为扁平形状,让人联想到机化性肺炎中的Ⅰ型肺泡上皮细胞,这一过程不同于UIP中紊乱或延迟的上皮化52,55(图1D)。肺泡上皮细胞恢复、肺泡毛细血管膜连续性恢复和肺泡单位完整性持续对于机化性肺炎的康复和修复似乎至关重要50,56,57,65。
第四,虽然机化性肺炎中的Masson小体与UIP中的成纤维细胞灶有一些共同的形态学特征,但这两种病程的结局明显不同51。在UIP中,成纤维细胞灶似乎驱动了不可逆的纤维化过程,而机化性肺炎中的纤维黏液样病变是可逆的。在机化性肺炎的纤维黏液样病变和UIP的成纤维细胞灶中,成纤维细胞增殖率是相似的。然而,与UIP相比,在机化性肺炎的肺泡内芽中,凋亡活性较高66。
第五,UIP和机化性肺炎在细胞外基质(ECM)的产生、沉积和蛋白质水解方面存在差异54,56。MMP和金属蛋白酶(TIMP)组织抑制物已知可调节ECM重构。在机化性肺炎中,MMP-2的凝胶溶解活性显著高于正常肺组织和UIP中54。在UIP中,肺结构被广泛重构,TIMP-2占主导地位,提示其在促进肺泡腔内ECM不可逆沉积方面发挥作用54,56。因此,机化性肺炎和UIP中增殖和凋亡的平衡差异39,67,68,以及MMP的存在对于机化性肺炎中纤维化病变的可逆性发挥了关键作用。
最后,在UIP中,由于结缔组织的持续沉积和肺泡塌陷,肺实质收缩并机械变形69。上述沉积和肺泡塌陷促发了在该疾病中观察到的永久性组织重构51,70。
临床表现
如果推定诊断为感染性肺炎的患者经过抗生素治疗无效,则常怀疑COP 6,9,13,27,36,47。COP的症状通常为亚急性,可在数周至数月期间出现7,9,20,22,33,34,44,47。患者常可准确记得疾病开始的时间。常见症状包括劳累时会加重的轻度至中度干咳(71%的报告病例)和呼吸困难(62%的报告病例)6-11,13,15,21,23,26,28-30,33-35,47。
据报道,10%~15%的病例出现流感样症状(即鼻塞、头痛、寒战和出汗、咽痛、咳嗽、疲劳、肌痛和发热)。44%的COP病例有发热。咯血的发生率很低(<5%)。
体格检查中最常见的发现是吸气性爆裂音(60%的报告病例)1,6-11,19,20,26,29,33,34,44,45。杵状指很少见(<3%的病例报告)。在不到5%的COP患者中,体格检查正常。
诊断性评估
我们需要采用多学科方法,结合临床、影像学和病理学专业知识来诊断COP2,3。
实验室检查
COP患者的实验室检查结果不具有特异性。然而,炎症标志物(如红细胞沉降率、C反应蛋白水平和白细胞计数)常升高6,7,9-11,21,23,27,30,33,34,37。机化性肺炎患者可能在出现相关结缔组织病前数周至数月就诊44。因此,如果怀疑结缔组织病,应针对这些疾病进行检测(如抗核抗体、类风湿因子、抗环瓜氨酸肽、肌酸激酶、抗拓扑异构酶[抗Scl-70]抗体、抗着丝粒抗体、抗双链DNA抗体,以及抗Jo-1抗体和其他抗合成酶抗体)44。
肺功能检查
肺功能检查结果常显示限制性通气障碍和一氧化碳弥散量降低1,6,8,9,14,21,26,29,34,36,47。在多达25%的COP患者中,肺容量正常11。除既往或当前吸烟的患者外,气流阻塞不是COP的表现6,7,24,71。疾病确诊时,肺部僵硬、无顺应性,在治疗有效的患者中,肺部可恢复正常71。休息和运动期间出现动脉低氧血症的情况常见8,9,11,14,21,23。
影像学检查
COP的影像学表现多种多样。COP患者的胸片通常有特征性表现,在肺容量正常的情况下,表现为双侧肺部斑片状或弥漫性、实变或薄雾样影1,6,8-10,20-22,26,38(图2A)。
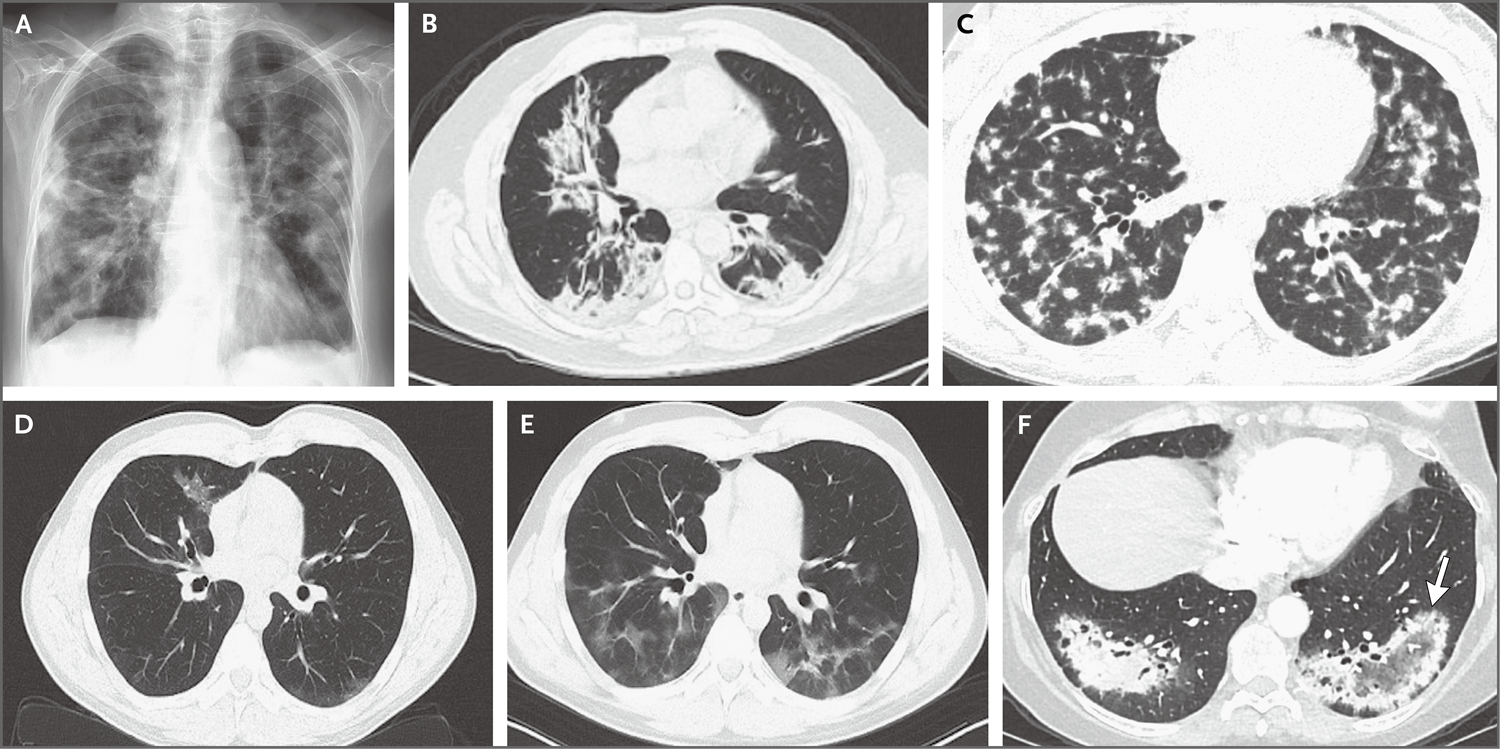
图A中的后前位胸片显示双侧弥漫性实变影,肺容量正常。图B中的胸部高分辨率CT(HRCT)扫描显示中、下叶周围和多灶实变。图C中的HRCT扫描显示弥漫性周围结节。图D和图E中的HRCT扫描显示移行性影;右上叶斑片状、毛玻璃样影(D),以及1个月后同一患者在新的区域出现斑片状、毛玻璃样影(图E)。图F中的HRCT扫描显示反晕征或环礁征,其特征是边缘实变,中心透明或毛玻璃样影(箭形)。
病变的范围和严重程度在高分辨率计算机断层(CT)肺部扫描中更为明显,通常比X线平片显示的病变更为广泛。高分辨率CT主要表现为周围和多灶实变(伴或不伴支气管充气征)10,14,23,26,29,33,34,41,45,47,72,73。上述发现可能为单侧,也可能为双侧。病变分布于所有肺区,胸膜下及下肺区分布略多14,44-46,72(图2B)。其他影像学发现包括毛玻璃样影;直径约为8 mm的结节(排列为界限清楚的腺泡状)或较小结节(排列更为稀疏,界限不清)74(图2C);支气管血管周围型,支气管血管束周围有实变区74;平行或垂直于胸膜的胸膜下线状和带状影73,74;以及局灶性病变14,33,72。病变偶尔呈小叶周围分布,以边界不清、弓形或多边形影为特征,以胸膜下为主,被充气肺包围73。影像学异常也可表现为伴有自发消退区和新实变区的移行性影4,7,9,20,21,23,34,36,41(图2D和2E)。反晕征(或环礁征)以边缘实变、中心透明或毛玻璃样影为特征,见于不到5%的病例,并且对机化性肺炎似乎具有相对特异性14,41,46,47,75(图2F)。纵隔淋巴结肿大的情况罕见14,46,47,72。据报道,少数病例有少量胸腔积液6,9,11,14,23,41,45,46,72,75。
在随访时的高分辨率CT检查中,实变与实质异常部分或完全消退相关,而网状影可持续或进展35,45。进行性纤维化和蜂窝状改变非常罕见59,72。虽然影像学发现存在差异,但相关临床背景下的双侧肺泡影可支持机化性肺炎的诊断。
支气管肺泡灌洗标本分析
如果怀疑COP,建议对支气管肺泡灌洗(BAL)标本进行分析,以排除感染和其他疾病,如嗜酸性肺炎和肺泡出血。BAL标本的细胞分析结果常显示淋巴细胞性肺泡炎,伴有中性粒细胞和嗜酸性粒细胞计数增加8,9,11,20-22,24,26,30,32,34,36,40,47,71,76。然而,存在这些细胞类型提示我们调查机化性肺炎的继发性原因(如过敏性肺炎、感染和嗜酸性肺炎)。BAL检查结果恢复正常的时间比临床和影像学检查结果改善的时间晚76。
组织病理学评估
COP常可在未经组织病理学确认的情况下进行治疗。然而,在某些病例中,可能需要通过组织检查来确认诊断。有关活检的决策应进行多学科讨论。组织学改变可能提示继发性机化性肺炎的基础病因(如误吸、血管炎或感染)60。在未行活检而采取治疗的病例中,如果临床随访结果与COP诊断不吻合,应重新评估,而且可能有必要进行活检。
COP患者肺活检标本的组织病理学检查结果显示腔内有疏松结缔组织栓子,累及肺泡腔和肺泡管,也可累及细支气管19(图3A和3B)。肺的基础结构保留。腔内疏松结缔组织栓子常以细柄连接到肺泡壁,并通过肺泡孔从一个肺泡延伸到相邻的肺泡,形成特征性的蝴蝶状结构52(图3C)。肺泡壁可出现轻度慢性炎症(如涉及淋巴细胞和浆细胞)。然而,观察到以下情况时,提示有其他诊断:显著的间质慢性炎症(涉及中性粒细胞或嗜酸性粒细胞77)、形态不良的肉芽肿、细支气管周围化生、淋巴样聚集、血管炎、间质纤维化或镜下蜂窝状改变。
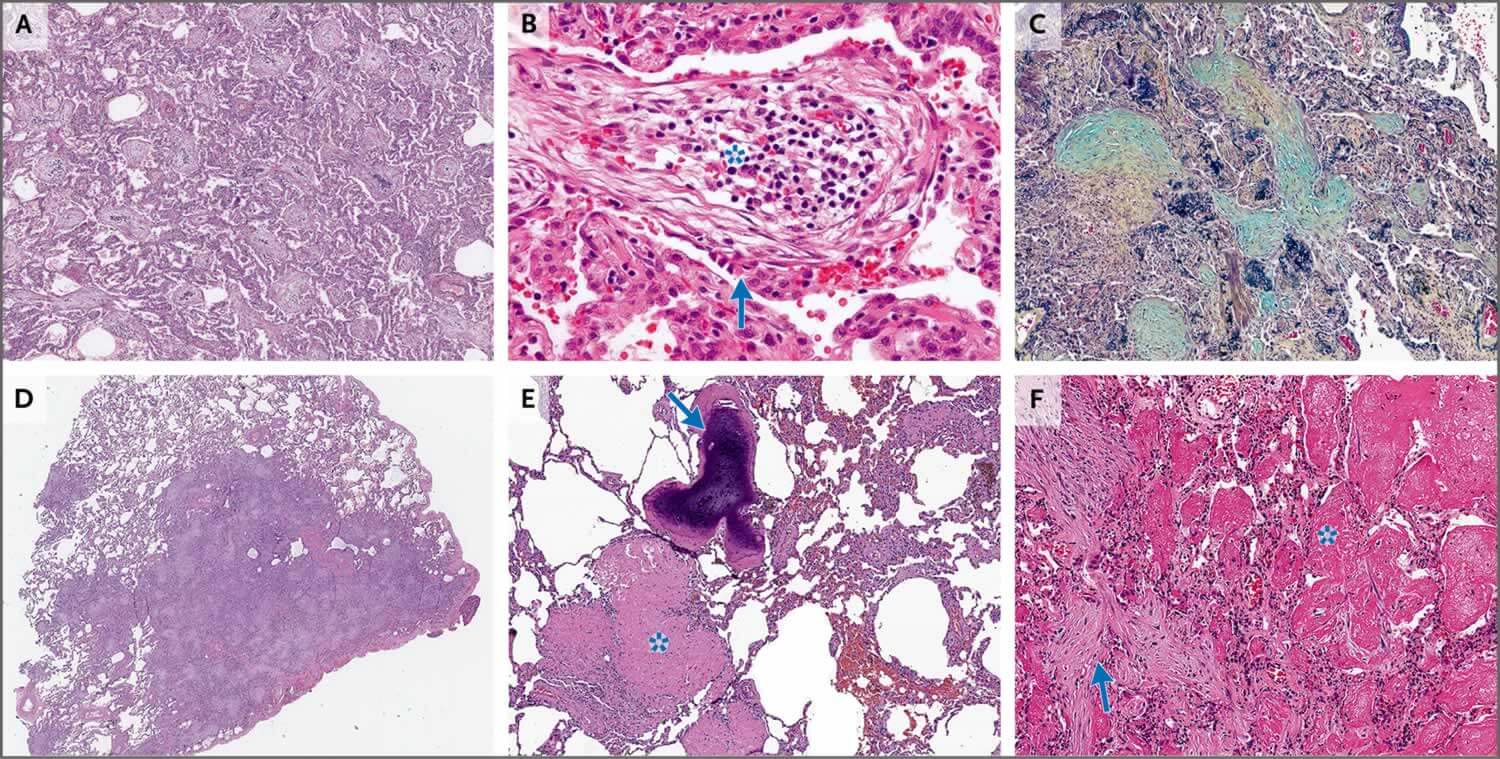
图A中低倍放大的显微照片(苏木精和伊红染色)显示腔内多个形状各异的疏松结缔组织栓子。其间的肺泡壁因炎症浸润而轻度增厚,但肺结构仍保留,无纤维化特征。图B中高倍放大的显微照片(苏木精和伊红染色)显示腔内纤维黏液样病变,有一簇炎症细胞(星号),再生上皮细胞(有些呈扁平形状,与Ⅰ型肺泡细胞一致)覆盖在芽的表面(箭形)。图C中高倍放大的显微照片(五色染色)显示腔内疏松结缔组织栓子(绿色),栓子通过肺泡孔从一个肺泡延伸到相邻的肺泡(蝴蝶状结构)。肺泡壁及周围实质有轻度炎症。图D中低倍放大的显微照片(苏木精和伊红染色)显示手术切除的局灶性机化性肺炎病变。图E中低倍放大的显微照片(苏木精和伊红染色)显示瘢痕机化性肺炎,伴有管腔密集透明化和纤维化栓子(星号)和化生骨形成(箭形),肺基础结构保留。图F中高倍放大的显微照片(苏木精和伊红染色)显示急性纤维素性机化性肺炎,其特征包括呈球状的肺泡内纤维蛋白(星号)和机化性肺炎的腔内纤维黏液样病变(箭形)。
机化性肺炎的组织学模式可通过小的活检标本(如经支气管或针穿活检标本)来识别。然而,标本越小,要识别组织学模式的所有特征就越困难。此外,小样本更有可能出现采样问题。因此,肺活检标本(包括手术标本)结果与CT表现之间的相关性很重要,它有助于确定活检标本可否代表间质病程6,13。有研究者建议使用连续分层切片对小活检标本进行显微镜下检查,以增加发现机化性肺炎组织学模式的机会78。
变型
局灶性机化性肺炎
局灶性机化性肺炎相对少见(见于<15%的COP患者),患者常无症状6,14,32,36,43,44(图3D)。单发病灶通常可通过手术切除治愈6,14,32,36,43,44。局灶性机化性肺炎必须与肺癌鉴别。
暴发性疾病
一部分机化性肺炎患者表现为快速进展的临床病程(例如,需要高流量吸氧和发展到机械通气)8,30,59。在这种情况下,必须排除继发性原因,特别是感染、结缔组织病、自身免疫病、药物或环境物质暴露、弥漫性肺泡损伤或间质性肺疾病急性加重59。排除感染后,建议静脉给予糖皮质激素治疗59。呼吸衰竭是死亡的主要原因,通常发生在住院后30~50日8,59。
瘢痕机化性肺炎
在一些机化性肺炎病例中,气腔充满松散的纤维黏液样结缔组织,伴有腔内致密嗜酸性纤维化形成,肺基础结构保留43,79。肺实质可见线状纤维带和化生骨形成区(树突状骨化)43,61,79(图3E)。瘢痕变异型似乎预示着纤维化非特异性间质性肺炎,这是一种更顽固的机化性肺炎,应该从形态学上与典型COP鉴别26,61,79。
急性纤维素性机化性肺炎
急性纤维素性机化性肺炎是一种罕见的肺泡填充性疾病,其特征是斑片状分布80,81(图3F)。这种变异型可为特发性,也可与其他病程(如弥漫性肺泡损伤、过敏性肺炎、感染、药物毒性、嗜酸性肺炎和结缔组织病)相关80-83。
鉴别诊断
COP的鉴别诊断包括具有类似临床和影像学特征的多种疾病。其中最重要的是社区获得性肺炎。通常情况下,抗生素治疗无效可提示COP。应考虑与影像学检查中波动性、多灶性实质实变相关的以下临床病程:过敏性肺炎(暴露于已知病原体)、嗜酸性肺炎(血液或肺泡嗜酸性粒细胞增多)、肺泡出血(咯血)和血管炎(存在抗中性粒细胞胞质抗体)。肺淋巴瘤和浸润性黏液腺癌的影像学表现可能与COP相似(斑片状、结节状实变区伴支气管充气征)。如果同时或序贯出现机化性肺炎和非特异性间质性肺炎的表现,应查找基础病因(如结缔组织病、抗合成酶综合征、过敏性肺炎或药物毒性)。
治疗
目前对COP采取的是经验性治疗,因为尚未开展前瞻性随机试验。启动治疗的决策与和治疗方案的选择取决于患者就诊时临床、生理和影像学异常的严重程度以及疾病进展的快慢。已有关于自发性改善的报道(见于<10%的患者),主要见于病情轻(症状少,病情程度有限)或者有禁忌证或拒绝治疗的患者1,10,11,14,20,21,23,32,35,44。
糖皮质激素治疗
对于COP导致呼吸障碍的有症状患者,全身糖皮质激素治疗是首选治疗方案8,9,14,23,24,26,30,44,71。常规起始剂量为每日0.5~1 mg/kg的泼尼松(根据理想体重计算剂量),最大剂量为每日60 mg(每日1次早晨口服)。以上述起始剂量用药2~4周。根据临床疗效将剂量逐渐降低至0.25 mg/kg,直至完成4~6个月治疗。在随后6~12个月,如果患者病情稳定或改善,则将口服糖皮质激素逐渐减量至停药。
糖皮质激素治疗通常可在24~72小时改善患者病情14,32。患者症状通常减少,之后,影像学表现在诊断后3个月内消退6,13,14,76。建议使用>20 mg/d剂量的泼尼松预防耶氏肺孢子虫感染。对于即将发生呼吸衰竭的重度或快速进展患者,可能需要大剂量甲泼尼松(每日静脉给药500~1,000 mg,用药3~5日)糖皮质激素治疗,病情改善(一般在数日内)后可转为口服治疗45。
据报道有不到25%的病例出现疾病复发(即症状恶化,或者糖皮质激素治疗期间或之后的胸部CT扫描显示特征性新影或残留影恶化),复发通常发生在最初就诊后1年内1,6,7,9-11,14,15,23,27,35,38,44,45。药物减量过快或停药过早时,可出现复发7,27,38,44。复发大多发生于泼尼松减量至≤15 mg/d后。有几个因素与复发相关:诊断时间延迟14,38;启动治疗时间延迟(出现症状>2个月后)38,45;重度疾病,包括多灶影9,42,44,46;胸部影像显示牵拉性支气管扩张45;一氧化碳弥散量异常(<预测值的50%)44;存在胆汁淤积38,48;低氧血症(动脉氧分压<70 mmHg)27;肺泡内纤维蛋白37,42或者背景肺实质瘢痕化和重构的组织病理学表现25。
复发的治疗方式通常是恢复糖皮质激素用药或增加剂量。一项研究表明,治疗复发时,小剂量糖皮质激素(≤20 mg/d)与大剂量相比,累积剂量较低,副作用较少,并且使用两种剂量的客观获益相似38。在COP患者中,复发与发病率或死亡率增加无关14,38,44,46。
其他治疗
对于全身糖皮质激素初始治疗未能改善病情,或者糖皮质激素无法逐渐减量至安全水平(无不可接受的副作用)的患者,可考虑其他治疗药物。
大环内酯类抗生素
病例报告和小规模回顾性病例系列研究提示,在COP患者中,具有抗炎特性的大环内酯类抗生素(如红霉素或克拉霉素)可作为口服糖皮质激素的辅助方案或替代方案1,11,28,44,84。大环内酯类抗生素通常用药3~6个月或更长时间,并在停止治疗期间密切监测,以防复发。遗憾的是,大环内酯类药物似乎不如糖皮质激素有效。
细胞毒性疗法
硫唑嘌呤或环磷酰胺不推荐用于COP患者,只有其他疗法均失败的极少数情况例外8,28,30,31,59,71。对于肾功能正常的患者,硫唑嘌呤的起始剂量为每日1~2 mg/kg(每日1次口服),最大剂量为每日150 mg。建议从每日50 mg的剂量开始,在2~4周期间缓慢增加剂量,治疗持续至少3个月。考虑到环磷酰胺的相关毒性作用,应在6个月后停药71。
吗替麦考酚酯和其他药物
吗替麦考酚酯是淋巴细胞增殖抑制剂,在纤维化肺疾病(包括COP)治疗中,越来越多地被用作糖皮质激素助减剂31,81。在病例报告中,环孢素85,86、利妥昔单抗87和静脉给予免疫球蛋白88也被用于治疗快速进展性疾病或糖皮质激素耐药性机化性肺炎(通常与糖皮质激素合用),并获得了有限的成功。
预后
COP患者的预后和治疗效果一般都很好。影像学上有气腔影的患者比有网状影的患者预后好得多23,25,35,46。对于住院患者,住院时间通常不到3周;疾病得到确诊并启动糖皮质激素治疗后,病情通常快速改善(通常在72小时内,很少>10日)14。
在机化性肺炎患者中,需要机械通气并导致死亡的进行性呼吸衰竭罕见6,16,30。在大多数回顾性研究中,因COP死亡的患者比例<10%,而且死亡原因通常与COP无关1,6-11,14,19-21,23-32,34-38,41-46。5年生存率超过90%。然而,COP患者的死亡率高于一般人群6,16。在继发性机化性肺炎患者中,死亡率较高,死因通常是基础疾病6,14,27。
未来方向
COP的发病率和患病率仍不明确。然而,鉴于我们对该疾病的定义已有所改进,在特发性间质性肺炎登记系统中持续前瞻性收集数据应该可以阐明上述问题。我们需要开展更多研究来区分原发性COP和继发性机化性肺炎。糖皮质激素的剂量和用药持续时间仍不明确,免疫抑制治疗作为初级或二级治疗的效果尚不清楚。如果可以理清机化性肺炎发病和消退的细胞和分子机制,那么对于UIP中持续进展且不可逆的纤维化病变,我们可能可以更好地确定危险因素和治疗策略。尤其是如果可以了解成纤维细胞灶和Masson小体之间的区别,我们可能可以为机化性肺炎和UIP制定更好的诊断和治疗方法。
作者信息Talmadge E. King, Jr., M.D., and Joyce S. Lee, M.D.
From the University of California, San Francisco (T.E.K.); and the University of Colorado Anschutz Medical Campus, Aurora (J.S.L.). Dr. King can be contacted at talmadge.king@ucsf.edu or at the School of Medicine, University of California San Francisco, 513 Parnassus Ave., Box 0410, San Francisco, CA 94143.
参考文献
1. Epler GR, Colby TV, McLoud TC, Carrington CB, Gaensler EA. Bronchiolitis obliterans organizing pneumonia. N Engl J Med 1985;312:152-158.
2. American Thoracic Society; European Respiratory Society. American Thoracic Society/European Respiratory Society international multidisciplinary consensus classification of the idiopathic interstitial pneumonias. This joint statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) was adopted by the ATS board of directors, June 2001 and by the ERS executive committee, June 2001. Am J Respir Crit Care Med 2002;165:277-304.
3. Travis WD, Costabel U, Hansell DM, et al. An official American Thoracic Society/European Respiratory Society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med 2013;188:733-748.
4. Davison AG, Heard BE, McAllister WA, Turner-Warwick ME. Cryptogenic organizing pneumonitis. Q J Med 1983;52:382-394.
5. Cottin V, Cordier J-F. Cryptogenic organizing pneumonia. Semin Respir Crit Care Med 2012;33:462-475.
6. Lohr RH, Boland BJ, Douglas WW, et al. Organizing pneumonia. Features and prognosis of cryptogenic, secondary, and focal variants. Arch Intern Med 1997;157:1323-1329.
7. Boots RJ, McEvoy JD, Mowat P, Le Fevre I. Bronchiolitis obliterans organising pneumonia: a clinical and radiological review. Aust N Z J Med 1995;25:140-145.
8. Chang J, Han J, Kim DW, et al. Bronchiolitis obliterans organizing pneumonia: clinicopathologic review of a series of 45 Korean patients including rapidly progressive form. J Korean Med Sci 2002;17:179-186.
9. Barroso E, Hernandez L, Gil J, Garcia R, Aranda I, Romero S. Idiopathic organizing pneumonia: a relapsing disease. 19 years of experience in a hospital setting. Respiration 2007;74:624-631.
10. Sveinsson OA, Isaksson HJ, Sigvaldason A, Yngvason F, Aspelund T, Gudmundsson G. Clinical features in secondary and cryptogenic organising pneumonia. Int J Tuberc Lung Dis 2007;11:689-694.
11. Drakopanagiotakis F, Paschalaki K, Abu-Hijleh M, et al. Cryptogenic and secondary organizing pneumonia: clinical presentation, radiographic findings, treatment response, and prognosis. Chest 2011;139:893-900.
12. Wang Y, Jin C, Wu CC, et al. Organizing pneumonia of COVID-19: time-dependent evolution and outcome in CT findings. PLoS One 2020;15(11):e0240347-e0240347.
13. Alasaly K, Muller N, Ostrow DN, Champion P, FitzGerald JM. Cryptogenic organizing pneumonia. A report of 25 cases and a review of the literature. Medicine (Baltimore) 1995;74:201-211.
14. Zhang Y, Li N, Li Q, et al. Analysis of the clinical characteristics of 176 patients with pathologically confirmed cryptogenic organizing pneumonia. Ann Transl Med 2020;8:763-763.
15. Vieira AL, Vale A, Melo N, et al. Organizing pneumonia revisited: insights and uncertainties from a series of 67 patients. Sarcoidosis Vasc Diffuse Lung Dis 2018;35:129-138.
16. Gudmundsson G, Sveinsson O, Isaksson HJ, Jonsson S, Frodadottir H, Aspelund T. Epidemiology of organising pneumonia in Iceland. Thorax 2006;61:805-808.
17. Karakatsani A, Papakosta D, Rapti A, et al. Epidemiology of interstitial lung diseases in Greece. Respir Med 2009;103:1122-1129.
18. Xaubet A, Ancochea J, Morell F, et al. Report on the incidence of interstitial lung diseases in Spain. Sarcoidosis Vasc Diffuse Lung Dis 2004;21:64-70.
19. Guerry-Force ML, Müller NL, Wright JL, et al. A comparison of bronchiolitis obliterans with organizing pneumonia, usual interstitial pneumonia, and small airways disease. Am Rev Respir Dis 1987;135:705-712.
20. Nagai S, Aung H, Tanaka S, et al. Bronchoalveolar lavage cell findings in patients with BOOP and related diseases. Chest 1992;102:Suppl:32S-37S.
21. Izumi T, Kitaichi M, Nishimura K, Nagai S. Bronchiolitis obliterans organizing pneumonia. Clinical features and differential diagnosis. Chest 1992;102:715-719.
22. Costabel U, Teschler H, Guzman J. Bronchiolitis obliterans organizing pneumonia (BOOP): the cytological and immunocytological profile of bronchoalveolar lavage. Eur Respir J 1992;5:791-797.
23. Yamamoto M, Ina Y, Kitaichi M, Harasawa M, Tamura M. Clinical features of BOOP in Japan. Chest 1992;102:Suppl:21S-25S.
24. Pesci A, Majori M, Piccoli ML, et al. Mast cells in bronchiolitis obliterans organizing pneumonia: mast cell hyperplasia and evidence for extracellular release of tryptase. Chest 1996;110:383-391.
25. Yousem SA, Lohr RH, Colby TV. Idiopathic bronchiolitis obliterans organizing pneumonia/cryptogenic organizing pneumonia with unfavorable outcome: pathologic predictors. Mod Pathol 1997;10:864-871.
26. Nagai S, Kitaichi M, Itoh H, Nishimura K, Izumi T, Colby TV. Idiopathic nonspecific interstitial pneumonia/fibrosis: comparison with idiopathic pulmonary fibrosis and BOOP. Eur Respir J 1998;12:1010-1019.
27. Watanabe K, Senju S, Wen FQ, Shirakusa T, Maeda F, Yoshida M. Factors related to the relapse of bronchiolitis obliterans organizing pneumonia. Chest 1998;114:1599-1606.
28. Basarakodu KR, Aronow WS, Nair CK, et al. Differences in treatment and in outcomes between idiopathic and secondary forms of organizing pneumonia. Am J Ther 2007;14:422-426.
29. Vasu TS, Cavallazzi R, Hirani A, Sharma D, Weibel SB, Kane GC. Clinical and radiologic distinctions between secondary bronchiolitis obliterans organizing pneumonia and cryptogenic organizing pneumonia. Respir Care 2009;54:1028-1032.
30. Yoo J-W, Song JW, Jang SJ, et al. Comparison between cryptogenic organizing pneumonia and connective tissue disease-related organizing pneumonia. Rheumatology (Oxford) 2011;50:932-938.
31. Todd NW, Marciniak ET, Sachdeva A, et al. Organizing pneumonia/non-specific interstitial pneumonia overlap is associated with unfavorable lung disease progression. Respir Med 2015;109:1460-1468.
32. Niksarlıoğlu EY, Özkan GZ, Bakan ND, Yurt S, Kılıç L, Çamsarı G. Cryptogenic organizing pneumonia: clinical and radiological features, treatment outcomes of 17 patients, and review of the literature. Turk J Med Sci 2016;46:1712-1718.
33. Yılmaz S, Akıncı Özyürek B, Erdoğan Y, et al. Retrospective evaluation of patients with organizing pneumonia: is cryptogenic organizing pneumonia different from secondary organizing pneumonia? Tuberk Toraks 2017;65:1-8.
34. Baha A, Yıldırım F, Köktürk N, et al. Cryptogenic and secondary organizing pneumonia: clinical presentation, radiological and laboratory findings, treatment, and prognosis in 56 cases. Turk Thorac J 2018;19:201-208.
35. Chung MP, Nam BD, Lee KS, et al. Serial chest CT in cryptogenic organizing pneumonia: evolutional changes and prognostic determinants. Respirology 2018;23:325-330.
36. Cordier JF, Loire R, Brune J. Idiopathic bronchiolitis obliterans organizing pneumonia: definition of characteristic clinical profiles in a series of 16 patients. Chest 1989;96:999-1004.
37. Yoshinouchi T, Ohtsuki Y, Kubo K, Shikata Y. Clinicopathological study on two types of cryptogenic organizing pneumonitis. Respir Med 1995;89:271-278.
38. Lazor R, Vandevenne A, Pelletier A, Leclerc P, Court-Fortune I, Cordier JF. Cryptogenic organizing pneumonia. Characteristics of relapses in a series of 48 patients. The Groupe d’Etudes et de Recherche sur les Maladles “Orphelines” Pulmonaires (GERM“O”P). Am J Respir Crit Care Med 2000;162:571-577.
39. Chung WY, Sun JS, Park JH, et al. Epithelial apoptosis as a clinical marker in idiopathic interstitial pneumonia. Respir Med 2010;104:1722-1728.
40. Jara-Palomares L, Gomez-Izquierdo L, Gonzalez-Vergara D, et al. Utility of high-resolution computed tomography and BAL in cryptogenic organizing pneumonia. Respir Med 2010;104:1706-1711.
41. Pardo J, Panizo A, Sola I, Queipo F, Martinez-Peñuela A, Carias R. Prognostic value of clinical, morphologic, and immunohistochemical factors in patients with bronchiolitis obliterans-organizing pneumonia. Hum Pathol 2013;44:718-724.
42. Nishino M, Mathai SK, Schoenfeld D, Digumarthy SR, Kradin RL. Clinicopathologic features associated with relapse in cryptogenic organizing pneumonia. Hum Pathol 2014;45:342-351.
43. Yousem SA. Cicatricial variant of cryptogenic organizing pneumonia. Hum Pathol 2017;64:76-82.
44. Zhou Y, Wang L, Huang M, et al. A long-term retrospective study of patients with biopsy-proven cryptogenic organizing pneumonia. Chron Respir Dis 2019;16:1479973119853829-1479973119853829.
45. Saito Z, Kaneko Y, Hasegawa T, et al. Predictive factors for relapse of cryptogenic organizing pneumonia. BMC Pulm Med 2019;19:10-10.
46. Cho YH, Chae EJ, Song JW, Do K-H, Jang SJ. Chest CT imaging features for prediction of treatment response in cryptogenic and connective tissue disease-related organizing pneumonia. Eur Radiol 2020;30:2722-2730.
47. Choi K-J, Yoo E-H, Kim KC, Kim EJ. Comparison of clinical features and prognosis in patients with cryptogenic and secondary organizing pneumonia. BMC Pulm Med 2021;21:336-336.
48. Spiteri MA, Klenerman P, Sheppard MN, Padley S, Clark TJ, Newman-Taylor A. Seasonal cryptogenic organising pneumonia with biochemical cholestasis: a new clinical entity. Lancet 1992;340:281-284.
49. Peyrol S, Cordier JF, Grimaud JA. Intra-alveolar fibrosis of idiopathic bronchiolitis obliterans-organizing pneumonia. Cell-matrix patterns. Am J Pathol 1990;137:155-170.
50. Myers JL, Katzenstein AL. Ultrastructural evidence of alveolar epithelial injury in idiopathic bronchiolitis obliterans-organizing pneumonia. Am J Pathol 1988;132:102-109.
51. Kuhn C, McDonald JA. The roles of the myofibroblast in idiopathic pulmonary fibrosis. Ultrastructural and immunohistochemical features of sites of active extracellular matrix synthesis. Am J Pathol 1991;138:1257-1265.
52. Basset F, Ferrans VJ, Soler P, Takemura T, Fukuda Y, Crystal RG. Intraluminal fibrosis in interstitial lung disorders. Am J Pathol 1986;122:443-461.
53. Kuhn C III, Boldt J, King TE Jr, Crouch E, Vartio T, McDonald JA. An immunohistochemical study of architectural remodeling and connective tissue synthesis in pulmonary fibrosis. Am Rev Respir Dis 1989;140:1693-1703.
54. Fukuda Y, Ishizaki M, Kudoh S, Kitaichi M, Yamanaka N. Localization of matrix metalloproteinases-1, -2, and -9 and tissue inhibitor of metalloproteinase-2 in interstitial lung diseases. Lab Invest 1998;78:687-698.
55. Lappi-Blanco E, Kaarteenaho-Wiik R, Salo S, et al. Laminin-5 gamma2 chain in cryptogenic organizing pneumonia and idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 2004;169:27-33.
56. Choi KH, Lee HB, Jeong MY, et al. The role of matrix metalloproteinase-9 and tissue inhibitor of metalloproteinase-1 in cryptogenic organizing pneumonia. Chest 2002;121:1478-1485.
57. Lappi-Blanco E, Kaarteenaho-Wiik R, Soini Y, Risteli J, Pääkkö P. Intraluminal fibromyxoid lesions in bronchiolitis obliterans organizing pneumonia are highly capillarized. Hum Pathol 1999;30:1192-1196.
58. Lee JW, Lee KS, Lee HY, et al. Cryptogenic organizing pneumonia: serial high-resolution CT findings in 22 patients. Am J Roentgenol 2010;195:916-922.
59. Cohen AJ, King TE Jr, Downey GP. Rapidly progressive bronchiolitis obliterans with organizing pneumonia. Am J Respir Crit Care Med 1994;149:1670-1675.
60. Beardsley B, Rassl D. Fibrosing organising pneumonia. J Clin Pathol 2013;66:875-881.
61. Churg A, Wright JL, Bilawich A. Cicatricial organising pneumonia mimicking a fibrosing interstitial pneumonia. Histopathology 2018;72:846-854.
62. Selman M, King TE, Pardo A. Idiopathic pulmonary fibrosis: prevailing and evolving hypotheses about its pathogenesis and implications for therapy. Ann Intern Med 2001;134:136-151.
63. Chilosi M, Caliò A, Rossi A, et al. Epithelial to mesenchymal transition-related proteins ZEB1, β-catenin, and β-tubulin-III in idiopathic pulmonary fibrosis. Mod Pathol 2017;30:26-38.
64. Selman M, Pardo A. From pulmonary fibrosis to progressive pulmonary fibrosis: a lethal pathobiological jump. Am J Physiol Lung Cell Mol Physiol 2021;321(3):L600-L607.
65. Lee JS, La J, Aziz S, et al. Molecular markers of telomere dysfunction and senescence are common findings in the usual interstitial pneumonia pattern of lung fibrosis. Histopathology 2021;79:67-76.
66. Lappi-Blanco E, Soini Y, Pääkkö P. Apoptotic activity is increased in the newly formed fibromyxoid connective tissue in bronchiolitis obliterans organizing pneumonia. Lung 1999;177:367-376.
67. Kuwano K, Kawasaki M, Maeyama T, et al. Soluble form of fas and fas ligand in BAL fluid from patients with pulmonary fibrosis and bronchiolitis obliterans organizing pneumonia. Chest 2000;118:451-458.
68. Ye Q, Dai H, Sarria R, Guzman J, Costabel U. Increased expression of tumor necrosis factor receptors in cryptogenic organizing pneumonia. Respir Med 2011;105:292-297.
69. McDonald JA. Idiopathic pulmonary fibrosis. A paradigm for lung injury and repair. Chest 1991;99:Suppl:87S-93S.
70. Myers JL, Katzenstein AL. Epithelial necrosis and alveolar collapse in the pathogenesis of usual interstitial pneumonia. Chest 1988;94:1309-1311.
71. King TE Jr, Mortenson RL. Cryptogenic organizing pneumonitis. The North American experience. Chest 1992;102:Suppl:8S-13S.
72. Lee KS, Kullnig P, Hartman TE, Müller NL. Cryptogenic organizing pneumonia: CT findings in 43 patients. Am J Roentgenol 1994;162:543-546.
73. Ujita M, Renzoni EA, Veeraraghavan S, Wells AU, Hansell DM. Organizing pneumonia: perilobular pattern at thin-section CT. Radiology 2004;232:757-761.
74. Oikonomou A, Hansell DM. Organizing pneumonia: the many morphological faces. Eur Radiol 2002;12:1486-1496.
75. Kim SJ, Lee KS, Ryu YH, et al. Reversed halo sign on high-resolution CT of cryptogenic organizing pneumonia: diagnostic implications. Am J Roentgenol 2003;180:1251-1254.
76. Costabel U, Teschler H, Schoenfeld B, et al. BOOP in Europe. Chest 1992;102:Suppl:14S-20S.
77. Olopade CO, Crotty TB, Douglas WW, Colby TV, Sur S. Chronic eosinophilic pneumonia and idiopathic bronchiolitis obliterans organizing pneumonia: comparison of eosinophil number and degranulation by immunofluorescence staining for eosinophil-derived major basic protein. Mayo Clin Proc 1995;70:137-142.
78. Nagata N, Hirano H, Takayama K, Miyagawa Y, Shigematsu N. Step section preparation of transbronchial lung biopsy. Significance in the diagnosis of diffuse lung disease. Chest 1991;100:959-962.
79. Woge MJ, Ryu JH, Bartholmai BJ, Yi ES. Cicatricial organizing pneumonia: a clinicopathologic and radiologic study on a cohort diagnosed by surgical lung biopsy at a single institution. Hum Pathol 2020;101:58-63.
80. Beasley MB, Franks TJ, Galvin JR, Gochuico B, Travis WD. Acute fibrinous and organizing pneumonia: a histological pattern of lung injury and possible variant of diffuse alveolar damage. Arch Pathol Lab Med 2002;126:1064-1070.
81. Bhatti S, Hakeem A, Torrealba J, McMahon JP, Meyer KC. Severe acute fibrinous and organizing pneumonia (AFOP) causing ventilatory failure: successful treatment with mycophenolate mofetil and corticosteroids. Respir Med 2009;103:1764-1767.
82. Lee SM, Park J-J, Sung SH, et al. Acute fibrinous and organizing pneumonia following hematopoietic stem cell transplantation. Korean J Intern Med 2009;24:156-159.
83. Lu J, Yin Q, Zha Y, et al. Acute fibrinous and organizing pneumonia: two case reports and literature review. BMC Pulm Med 2019;19:141-141.
84. Stover DE, Mangino D. Macrolides: a treatment alternative for bronchiolitis obliterans organizing pneumonia? Chest 2005;128:3611-3617.
85. Lee J, Cha SI, Park TI, Park JY, Jung TH, Kim CH. Adjunctive effects of cyclosporine and macrolide in rapidly progressive cryptogenic organizing pneumonia with no prompt response to steroid. Intern Med 2011;50:475-479.
86. Koinuma D, Miki M, Ebina M, et al. Successful treatment of a case with rapidly progressive bronchiolitis obliterans organizing pneumonia (BOOP) using cyclosporin A and corticosteroid. Intern Med 2002;41:26-29.
87. Shitenberg D, Fruchter O, Fridel L, Kramer MR. Successful rituximab therapy in steroid-resistant, cryptogenic organizing pneumonia: a case series. Respiration 2015;90:155-159.
88. Dimala CA, Patel U, Lloyd B, et al. A case report of steroid-resistant cryptogenic organizing pneumonia managed with intravenous immunoglobulins. Case Rep Pulmonol 2021;2021:9343491-9343491.
特别申明:本文为转载文章,转载自医学前沿,不代表贪吃的夜猫子立场,如若转载,请注明出处:https://www.nejmqianyan.cn/article-info?permalinks=YXQYra2116777
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫