急性肾损伤(AKI)是肝硬化患者的常见病。AKI发生于高达50%的住院肝硬化患者和58%的重症监护病房(ICU)肝硬化患者1-5。AKI具有高致病率和死亡率,并且与肝移植后慢性肾脏病(CKD)发病率增加相关1-3,5,6。进展至AKI晚期(表1)预示着预后更差1,2,5。
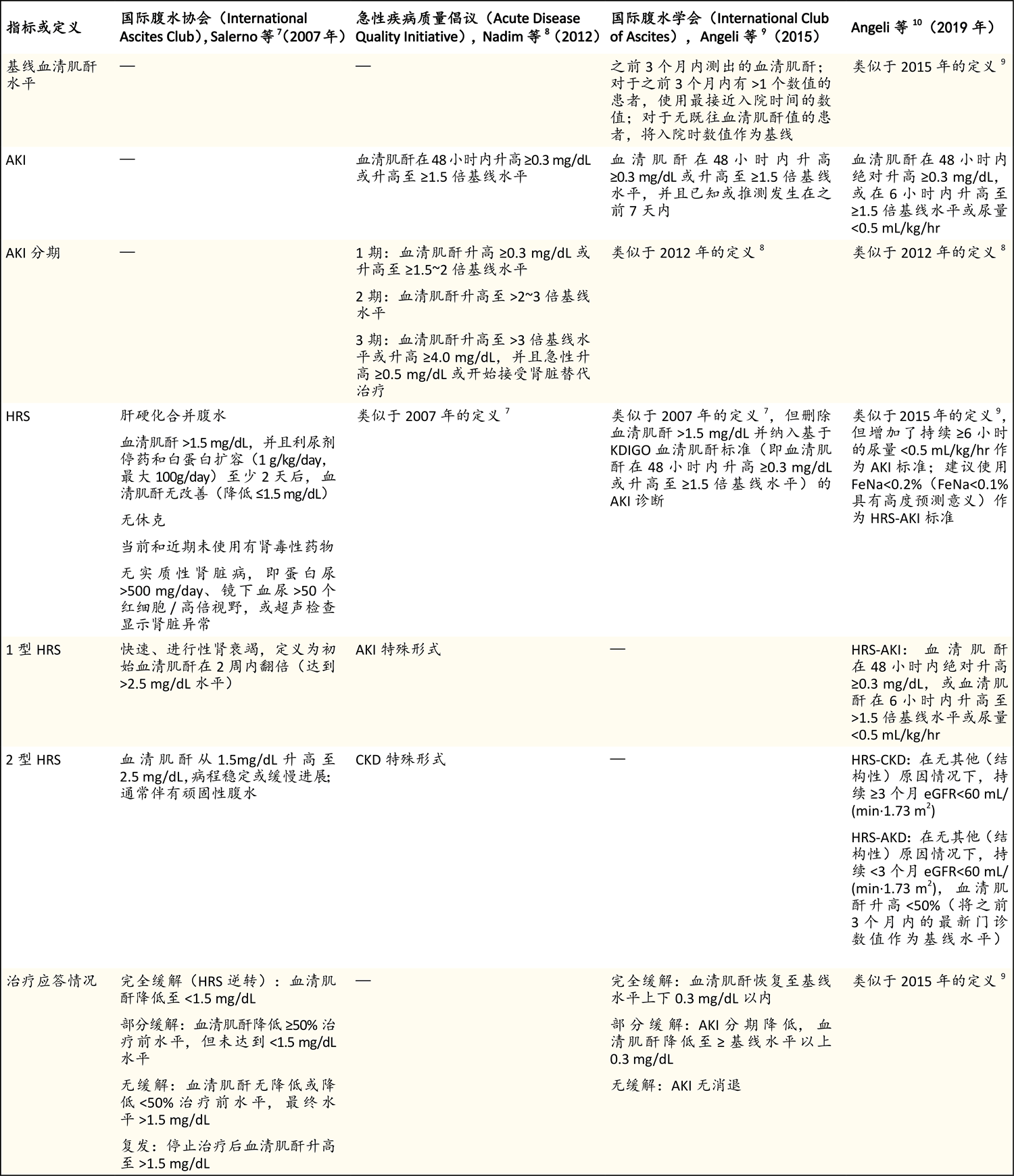
将肌酐数值转换为μmol/L需乘以88.4。CKD表示慢性肾脏病,eGFR表示估计肾小球滤过率,FeNa表示钠排泄分数,KDIGO表示改善全球肾脏病预后组织。
一般而言,AKI的三个主要原因11是肾灌注不足(也称为肾前性AKI,大多由血容量不足所致),肾性结构性肾损伤以及尿路梗阻引起的肾后性肾损伤。肝硬化患者肾灌注不足引起AKI的一个独特原因是肝肾综合征(HRS),这是肾血管收缩的结果。血容量不足引起的灌注不足约占肝硬化患者AKI病例的一半,肾脏原因(如急性肾小管坏死)约占30%,HRS约占15~20%,其中不到1%的病例可归因于肾后尿路梗阻3。
AKI和HRS的定义
2012年之前尚无肝硬化患者AKI定义标准,而HRS的定义为发生于肝硬化和门静脉高压患者的综合征,其特征为在无基础肾脏病的情况下出现肾功能不全(定义为血清肌酐水平>1.5 mg/dL[132.6 μmol/L])7。临床上将HRS分为1型(HRS-1)和2型(HRS-2),1型的特征为肾功能迅速下降,血清肌酐在不到2周时间内升高至超过2.5 mg/dL[221.0 μmol/L]水平,2型的特征为肾功能更缓慢下降。
在过去十年间,肝硬化患者的AKI和HRS定义做出了修订(表1)8-10。AKI的新定义与改善全球肾脏病预后组织(Kidney Disease: Improving Global Outcomes)的定义统一,即血清肌酐水平在48小时内升高≥0.3 mg/dL(26.5 μmol/L),或血清肌酐水平升高至≥1.5倍基线水平,并且已知或推测发生在之前7天内8-10,12。HRS的新定义删除了血清肌酐水平阈值(1.5 mg/dL),从而可以更早诊断和治疗血清肌酐水平正常但肾功能降低的患者,如女性、老年患者或少肌症患者。HRS的急性形式HRS-1也更名为HRS-AKI,目的是区别于更慢性形式HRS-2,后者现更名为HRS-CKD10。AKI定义中应考虑尿量变化,尤其是对于危重症肝硬化患者,现已证明在该人群中,尿量变化是AKI的灵敏、早期指标,并且与较差结局相关(表1)5,10,13。HRS定义的主要局限性之一是排除了基础实质性肾脏病。在非酒精性脂肪性肝炎发病率不断升高的时代,糖尿病、高血压或这两种疾病导致基础CKD的情况也在增加。在已确诊CKD的患者中,HRS-AKI的预后和治疗意义仍有待明确,这些意义可能与进展为HRS-CKD的HRS-AKI患者不同8,10。
病理生理学
肝硬化患者,尤其是有腹水的肝硬化患者,由于门静脉高压引起的血流动力学改变,AKI易感性增加(图1)14,15。门静脉高压发病机制中的初始机制是肝结构扭曲(纤维化和结节)导致肝内阻力增加和肝内血管张力增加。之后,内脏循环中血管扩张物质(最重要的是一氧化氮)被激活,进而导致内脏和全身血管进行性扩张。肠道菌群失调、细菌过度生长和紧密连接蛋白改变导致的细菌和细菌产物移位增多进一步引起血管扩张,进而导致有效动脉血容量减少,这样会激活神经体液系统(肾素-血管紧张素-醛固酮、交感神经和精氨酸-血管升压素系统),最终导致水钠潴留和腹水形成16,17。在肝硬化晚期,进行性血管扩张导致更严重的水潴留和钠潴留,二者分别导致顽固性腹水和稀释性低钠血症(图1)。
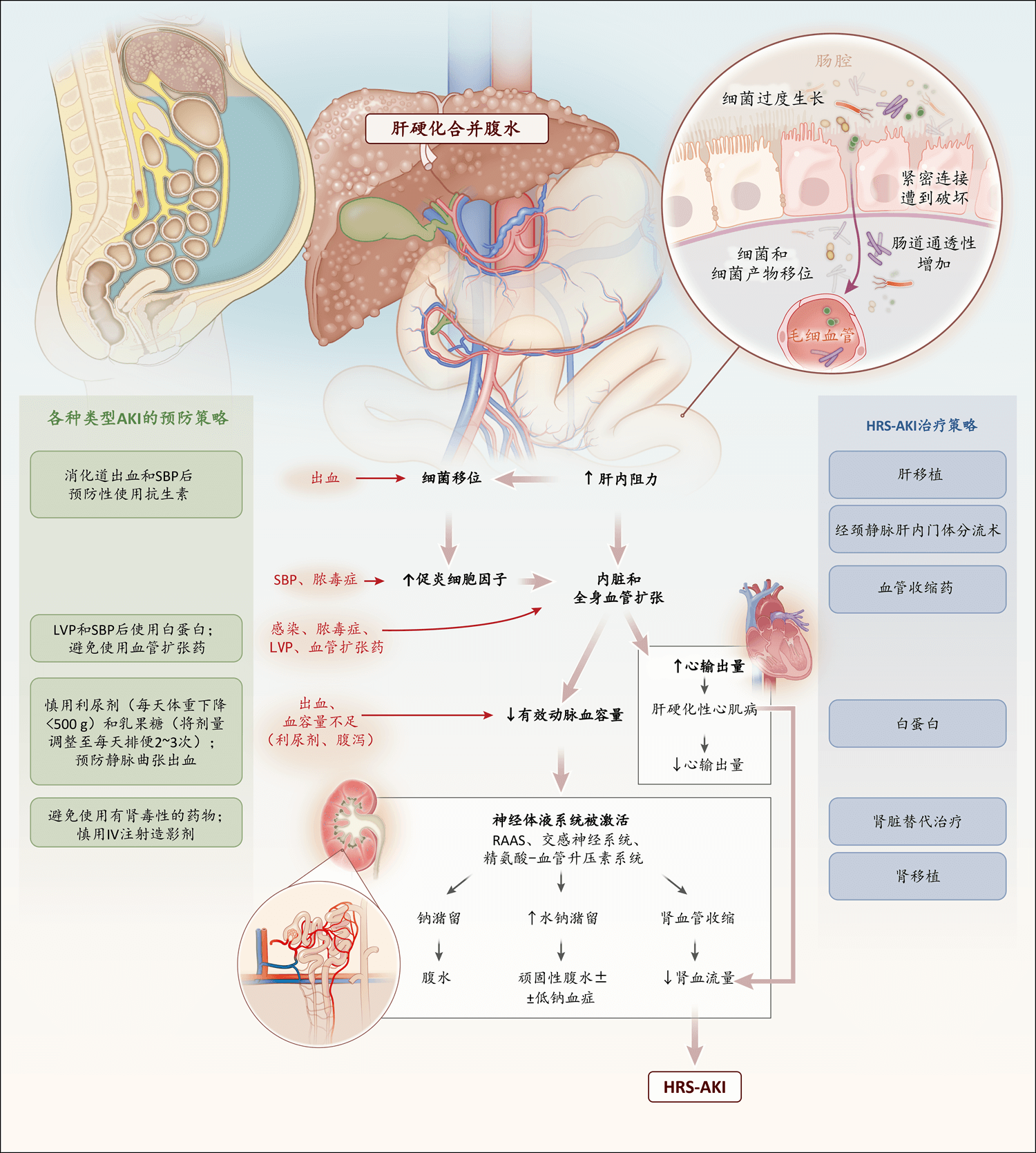
发生HRS-AKI的必要条件是有腹水,腹水通常为张力性腹水,且常伴有低钠血症、平均动脉压低和少尿。图中用红色箭头表示在肝硬化(即使无腹水)或HRS-AKI患者中,促发AKI的因素。图中显示了肝硬化患者各种类型AKI(包括HRS-AKI)的预防策略。IV表示静脉内,LVP表示大量放腹水,RAAS表示肾素-血管紧张素-醛固酮系统,SBP表示自发性细菌性腹膜炎。
随着进行性血管扩张,血管收缩系统(主要是肾素和血管紧张素)被激活,导致肾血管收缩和肾血流量减少。此外,在心力衰竭的这一高输出状态下(即所谓的肝硬化性心肌病),心输出量相对减少可能进一步导致肾灌注减少18-20。肾血流量减少导致肾小球滤过率(GFR)降低及扩容无效的肾前性肾损伤,即HRS-AKI。肝硬化患者的肾血管收缩无法通过释放血管扩张物质(如前列腺素)来逆转,原因是它们的生成减少和血管收缩物质(如内皮素)的局部释放。
肝硬化患者肾血管收缩和肾血流量减少的发病机制(“肝肾生理学”)是最初导致腹水的一系列机制。因此,有腹水(尤其是顽固性腹水)的肝硬化患者不仅发生AKI的风险最高,而且发生临床最严重形式HRS-AKI的风险也最高(图1)。虽然HRS-AKI可在无促发因素的情况下发生,但更常见的情况是由导致有效动脉血容量减少的因素促发。这些因素包括快速失水(如过度利尿或消化道出血)、药物(如血管紧张素转换酶抑制剂)引起的血管扩张加重以及全身炎性反应(如感染)(图1)。在肝硬化患者中,并非所有AKI病例都是由肾灌注不足导致,一些病例可能是由结构性肾损伤引起。然而,当肾脏灌注不足持续时间长或伴有“二次打击”(如暴露于肾毒性药物)时,肾脏灌注不足可能会导致结构性肾损伤,进而导致肾恢复延迟。
肾功能评估
肝硬化患者的肾功能评估仍然是一个至关重要且具有挑战性的问题。血清肌酐水平是最实用和最常用的肾功能指标,也是终末期肝病模型(Model for End-Stage Liver Disease,MELD)评分中用于确定等待肝移植患者优先顺序的指标,但血清肌酐会高估肝硬化患者的GFR,原因是肝病导致的肌酐生成减少、蛋白质-热量营养不良和肌肉萎缩。此外,在AKI合并液体超负荷患者中,即使GFR降低,血清肌酐水平升高也可能滞后数小时至数天21,22。外源性物质(如菊粉和碘酞酸盐[iothalamate])清除率指标不易获得,且会因腹水和细胞外容量扩张所致分布容量变化而造成差错。通过定时收集尿液(通常是24小时)获得的肌酐清除率测定值可能不准确,原因是尿液收集过程发生差错(收集不完全或收集过度),或者随着GFR下降,肾小管分泌排泄的肌酐增多。
基于血清肌酐、胱抑素C或两者的估计GFR(eGFR)计算公式是确定血清肌酐水平稳定人群肾功能的简单方法。然而,在肝硬化患者中,eGFR公式往往会将真实GFR高估10~20 mL/(min·1.73 m2),尤其是在GFR低于40 mL/(min·1.73 m2)、有腹水或有这两种情况的患者中,因此应谨慎使用23-25。eGFR值准确性对于肝硬化患者尤为重要,因为eGFR是确定患者是否适合肝肾联合移植的因素之一。最近建议从所有eGFR公式中删除种族这一项,这是消除肾脏病患者医疗差距的一个重要举措26,删除种族的建议已经被移植医学界采纳,然而,eGFR公式的这一更改对肝肾联合移植资格判断的影响仍有待充分研究27。
AKI的诊断检查和治疗
一旦诊断出AKI,一定要停用所有可能促发或加重AKI的药物(具体包括利尿剂、血管扩张药、非选择性β受体阻滞剂、非甾体抗炎药),并排除感染,尤其是自发性细菌性腹膜炎,这通常是AKI和HRS-AKI的促发因素(图2)。与此同时,AKI诊断检查对于治疗早期AKI和预防进展(AKI进展与死亡率增加相关)至关重要1,2,5。AKI病因是根据以下几项确定:患者病史和体格检查、尿液检查、利尿剂停药反应,以及临床适合情况下进行的液体冲击试验(volume challenge)(图2)。尿沉渣显微镜检查对于排除AKI的肾脏原因非常重要。
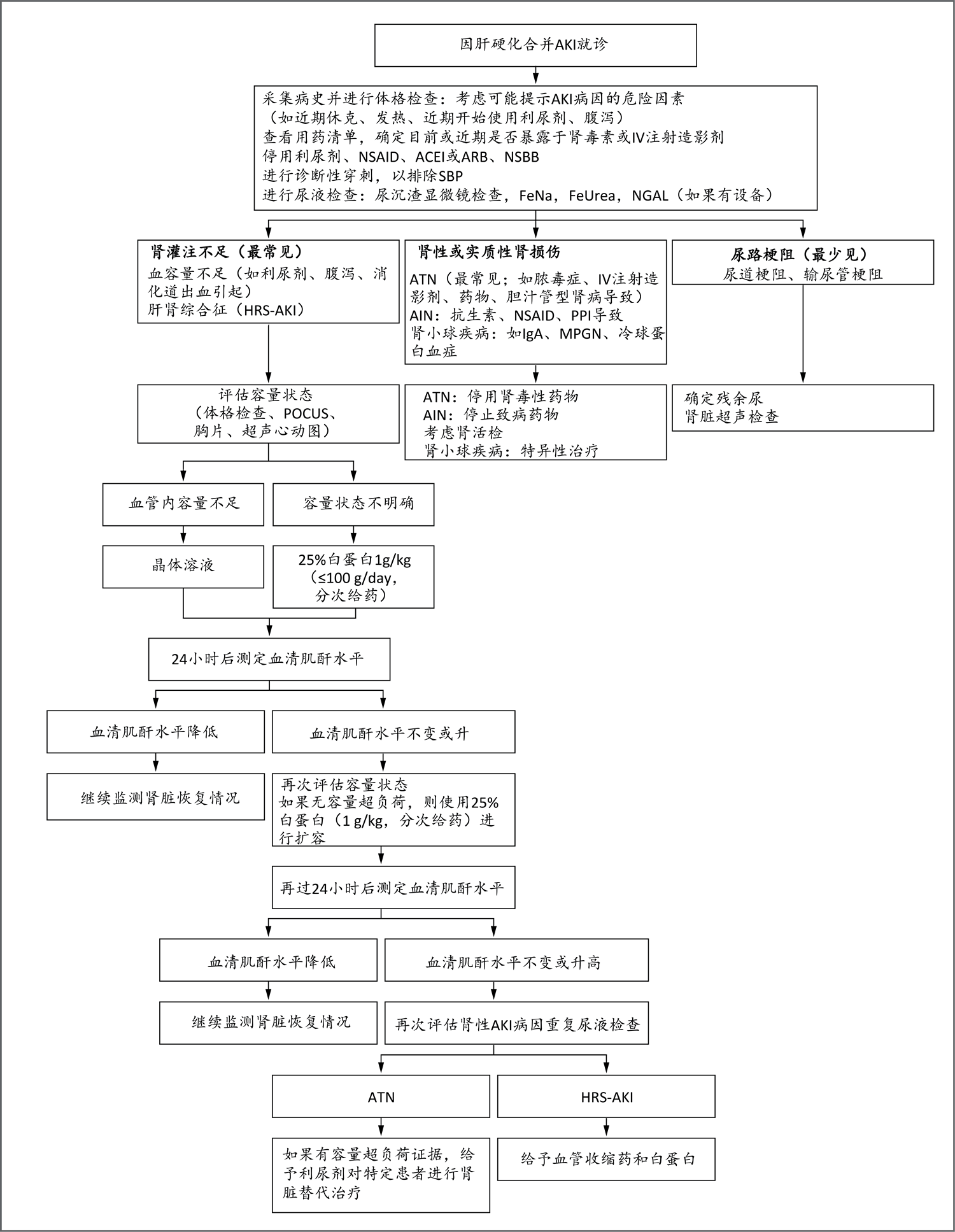
AKI的定义是血清肌酐水平在48小时内超过基线水平0.3 mg/dL(26.5 mmol/L),或血清肌酐水平≥1.5倍基线水平(已知或推测上述升高发生在之前7天内),或持续6小时的尿量<0.5 mL/kg/hr。尿液检查对于区分HRS-AKI和肾性或实质肾损伤所致AKI的各种原因非常重要。提示HRS-AKI的检查结果包括:尿沉渣正常,钠排泄分数(FeNa)低于0.1%,尿素排泄分数(FeUrea)低于21%。尿中性粒细胞明胶酶相关脂质运载蛋白(NGAL)水平高于220~244 μg/g肌酐提示急性肾小管坏死(ATN)。以下各项提示容量超负荷:全身性水肿、颈静脉扩张、胸片显示肺充血或右心室收缩压升高。如果有容量超负荷证据,可能需要开始或继续使用利尿剂。ACEI表示血管紧张素转换酶抑制剂,AIN表示急性间质性肾炎,ARB表示血管紧张素受体阻滞剂,MPGN表示膜增生性肾小球肾炎,NSAID表示非甾体抗炎药,NSBB表示非选择性β受体阻滞剂,POCUS表示床旁超声,PPI表示质子泵抑制剂。
临床医师通过钠和尿素排泄分数测定值来确认血容量不足和HRS-AKI,以及排除急性肾小管坏死。然而,肝硬化合并腹水患者已经有严重钠潴留,钠排泄分数低于1.0%在此类患者中常见,即使患者并无AKI28。因此,区分HRS-AKI和急性肾小管坏死往往有难度。一般而言,钠排泄分数低于0.1%、尿素排泄分数低于21%、尿白蛋白低于44 mg/dL这些临界值有助于确认HRS-AKI并排除急性肾小管坏死28-30。但应谨慎解读这些临界值,而且一定要结合患者临床表现进行解读,因为它们的灵敏度和特异性都不是很高,并且与组织学检查结果没有相关性。尿中性粒细胞明胶酶相关脂质运载蛋白是肾小管损伤的标志物,已被证明可用于鉴别HRS-AKI和急性肾小管坏死。然而,由于缺乏标准化、临界值不明确以及许多国家无法测定这一生物标志物,其在临床实践中的应用受到了限制28,31-34。只有结果可能改变治疗方案(如肾小球疾病的治疗)时,才应考虑肾活检,因为活检有创,可能发生出血并发症。
扩容是逆转血容量不足所致AKI的核心措施,扩容的效果有助于确定AKI病因(图2)。应根据AKI病因和患者容量状态个体化选择复苏液体类型(晶体溶液 vs. 白蛋白)和用量(图2)。对于临床上血容量不足或血容量正常的患者,建议尝试进行24~48小时的容量复苏。但是,对AKI患者补液时务必小心,要避免液体超负荷和肺水肿。评估血管内容量和容量反应性是可取方法,但有难度,因为许多血流动力学工具尚未在肝硬化患者中进行研究,而且由于腹水导致腹内压升高,可能会产生误导13。在一项小型、单中心、回顾性研究中,研究者采用床旁超声评估了诊断为HRS-AKI且被认为适当补液的患者的容量状态,结果发现21%的患者有血管内液体超负荷,28%的患者仍然有血管内容量不足35。应通过综合评估(包括详细采集病史和体格检查、床旁超声以及静态和动态测定[如果有设备])来判断容量状态和液体反应性。
尚无充分证据支持通过放腹水来改善肝硬化合并AKI患者的腹内压(以及理论上改善肾功能)。对于张力性腹水患者,为了提高其舒适度,建议放出部分腹水,并且静脉注射白蛋白,以防出现循环功能障碍。循环功能障碍是大量放腹水(放腹水>5升)后出现的一种血管扩张状态,可导致肾功能恶化36-38。
HRS-AKI的治疗
对于肝硬化患者,只有检查并排除AKI的其他原因后,才能启动HRS-AKI治疗(图2)。
药物治疗
HRS-AKI药物治疗主要使用血管收缩药联合静脉注射白蛋白(图3)39,40。作为概念验证,血清肌酐水平变化与血管收缩药引起的平均动脉压变化呈负相关41。目前尚未证明血管收缩药可延长生存期,因此应将其视为移植前的过渡治疗,而不是HRS-AKI的治愈方案。
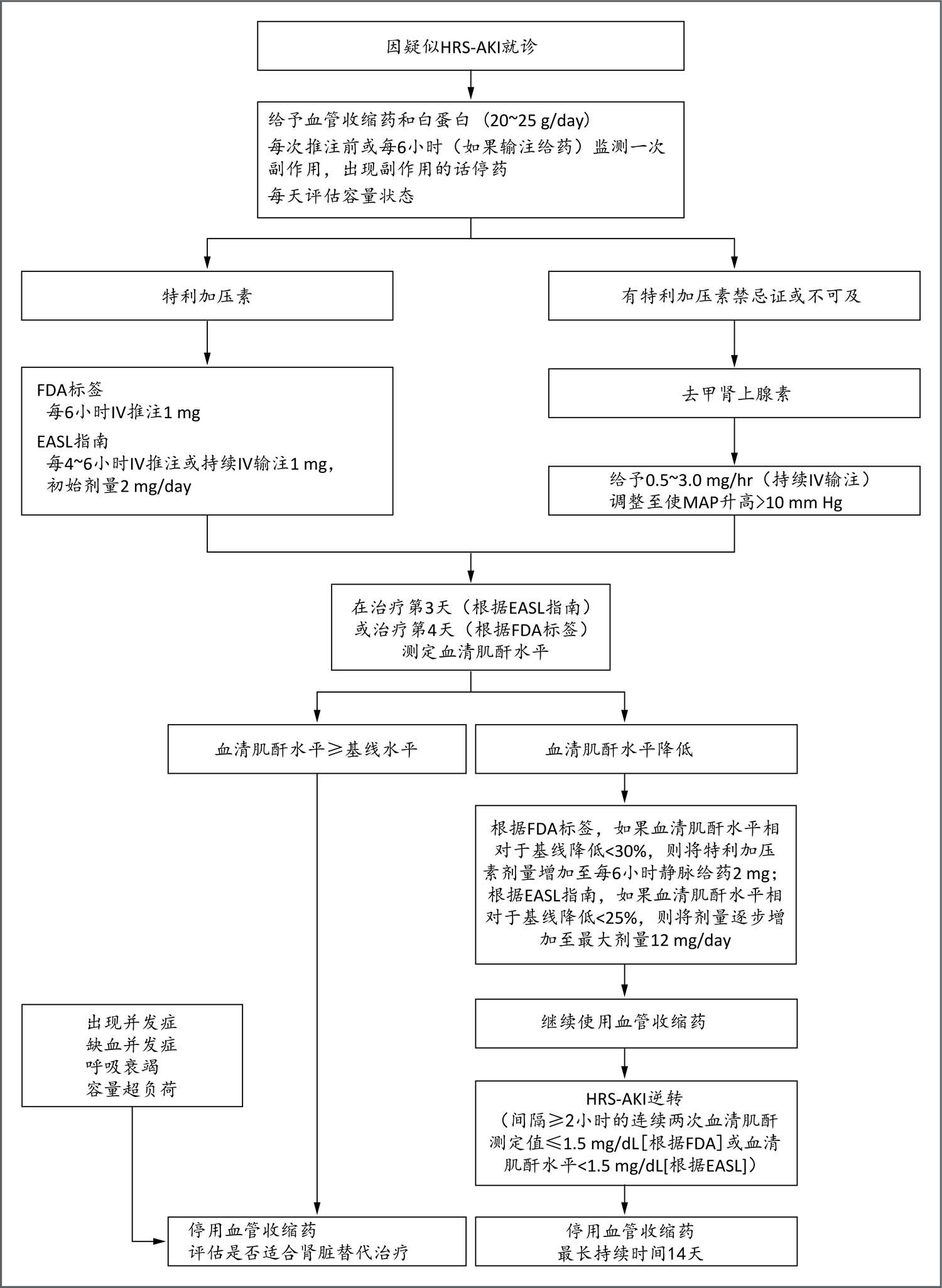
美国食品药品管理局(FDA)标签和欧洲肝脏研究学会(European Association for the Study of the Liver,EASL)38指南建议将特利加压素作为HRS-AKI一线治疗药物。副作用包括心肌梗死、外周或肠系膜缺血和肺水肿。应减少白蛋白输注量,对于有血管内容量超负荷证据的患者,建议慎用特利加压素。如果血氧饱和度(SpO2)低于90%,应暂停使用特利加压素。去甲肾上腺素用药仅限于重症监护病房(ICU)患者,需放置中心导管。如果有特利加压素禁忌证或不可及,可考虑将去甲肾上腺素作为替代方案。去甲肾上腺素副作用包括缺血事件和心脏节律障碍。如果特利加压素不可及或有禁忌证,并且无法转入ICU输注去甲肾上腺素,可考虑联用米多君(7.5~15 mg,口服,每日三次)和奥曲肽(100~200 μg,皮下注射,每日三次),用药时间24~48小时。米多君可能引起心动过缓。基线血清肌酐水平指的是血管收缩药开始用药前即刻测定的水平。MAP表示平均动脉压。
特利加压素是血管升压素类似物,也是全球最常用的血管收缩药,美国37和欧洲38指南均建议将其作为HRS-AKI一线治疗药物。特利加压素可静脉推注或持续输注,两种方式的疗效相似。然而,持续输注的累积日剂量和不良事件发生率较低42。可根据应答(血清肌酐水平变化)将初始剂量提高、维持或停药(图3)。在一项证明特利加压素对HRS-AKI患者疗效的大型随机对照试验中(该试验使特利加压素在美国获批),该药物与肺水肿引起的呼吸衰竭发生率增加相关43。因此,如果有血管内容量超负荷的临床证据(即全身性水肿、颈静脉扩张、低氧血症、胸片显示肺充血或超声心动图显示右心室收缩压升高),则须暂停使用特利加压素和白蛋白。
小型单中心研究显示,患者对去甲肾上腺素(替代性血管加压药)的应答与对特利加压素的应答相似。但去甲肾上腺素需要在ICU内持续输注39,40。联用奥曲肽和米多君具有较弱血管收缩活性,一项随机对照试验显示,在逆转HRS-AKI方面,联合治疗的效果劣于特利加压素44。因此,奥曲肽和米多君只能临时使用(用药24~48小时),并且只能在特利加压素不可及或有禁忌证的情况下使用。
经颈静脉肝内门体分流术
门静脉高压患者的一个重要治疗方案是经颈静脉肝内门体分流术(TIPS),TIPS可通过重新分配血容量和降低门静脉压力的方式改善肾功能45-48。对9项小型研究进行的荟萃分析提示,TIPS可显著改善肾功能,HRS-AKI患者的总缓解率为93%49。然而,目前尚无充分证据推荐使用TIPS治疗HRS-AKI。
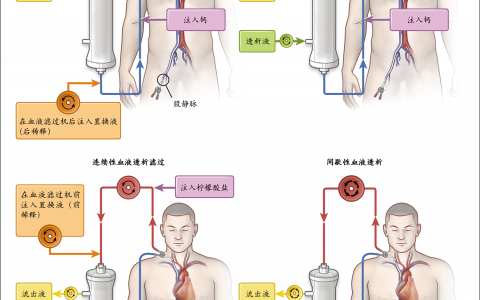
肾脏替代治疗
肾脏替代治疗被视为肝移植前的过渡治疗,但对于不适合肝移植的HRS-AKI患者,肾脏替代治疗因其高死亡率而存在争议50。然而,由于在HRS-AKI患者与肝硬化合并急性肾小管坏死患者中,肾脏替代治疗的相关死亡率相似51,因此可考虑在特定HRS-AKI患者中开展肾脏替代治疗试验13,37。对于肝硬化合并AKI患者应何时启动肾脏替代治疗,目前尚未达成共识。尽管几项随机对照试验并未显示对ICU危重患者人群早期启动肾脏替代治疗有益,但肝硬化患者在这些研究中被排除或占比很低52-55。因此,对于肝硬化患者,应根据药物治疗无效的危及生命适应证(如高钾血症、酸中毒或液体超负荷)、尿毒症并发症、肾功能轨迹或总体预后,个体化决定何时启动肾脏替代治疗13,37,56,57。
肝移植
肝移植是HRS-AKI患者的首选治疗方案。肝肾联合移植是肝移植前长期肾功能不全患者的一种潜在治疗方案,因为这些患者肾功能恢复的可能性低于短期肾功能不全患者。然而,目前仍然很难预测使得肾功能不太可能恢复的肾功能不全严重程度和持续时间6,58。2017年,美国器官获取和移植网络(Organ Procurement and Transplantation Network)根据之前的美国指南制定了肝肾联合移植标准。这些标准包括长期患AKI并接受透析以及患CKD等因素。该组织还实施了一项安全网政策,优先考虑肝移植后有持续重度肾功能不全的患者,使其可以在第一年内接受肾移植59,60。肾活检可能有助于确诊肾功能不全并确定其可逆性,以及确定是否需要肝肾联合移植61。我们需要移植后AKI可逆性的预测因素(如生物标志物),从而指导移植肾的分配62,63。
AKI的预防
AKI是肝硬化患者常见而严重的并发症。因此,当务之急是识别和管理可能导致AKI的事件,尤其是对于腹水患者(图1)64。应避免血容量不足,措施包括谨慎使用利尿剂(目标为每天体重下降<1 lb [0.45 kg])、谨慎使用乳果糖(将剂量调整至每天排便两或三次)和预防静脉曲张出血65。静脉输注白蛋白(剂量为每放出1 L腹水输注4~6 g白蛋白)已被证明可在大量放腹水(放出>5 L)后改善循环功能障碍,并预防AKI66。输注白蛋白还可降低自发性细菌性腹膜炎患者的AKI发生率和死亡率67。然而,在一项纳入自发性细菌性腹膜炎外其他感染患者的研究中,静脉输注白蛋白未能预防AKI,而且实际上与肺水肿发生率增加相关68。关于在门诊长期(每周或每2周一次)静脉输注白蛋白的结果,目前有争议。一项开放标签、随机、对照试验显示,该方法与腹水并发症(包括AKI)和死亡的发生率降低相关69,而一项随机、安慰剂对照试验显示,长期输注白蛋白未能显著降低AKI或死亡的发生率70。在一项纳入住院患者的随机对照试验中,静脉输注白蛋白(旨在将血清白蛋白水平维持在约3 g/dL)并未改善结局(其中一项是发生AKI),且与肺水肿发生率增加相关71。因此,目前不建议对门诊或住院患者长期输注白蛋白。
多种药物(如非甾体抗炎药和肾素-血管紧张素-醛固酮系统阻滞剂)可减少肾内血流量,进而产生直接肾毒性。部分药物(如放射造影剂、氨基糖苷类、万古霉素、两性霉素B)具有直接肾小管毒性,一些药物(如β-内酰胺类抗生素、质子泵抑制剂)可引起过敏性间质损伤。因此,在肝硬化合并腹水患者接受上述药物期间,应密切监测肾功能。目前缺乏这些患者静脉注射造影剂的数据。建议谨慎使用静脉注射造影剂,尤其是eGFR低于45 mL/(min·1.73 m2)的患者72。
结论
过去十年在肝硬化患者AKI分类、理解病理生理学、诊断和治疗方面取得的进展有助于我们更早诊断和治疗HRS-AKI。由于之前对HRS-AKI治疗开展的研究采用的是血清肌酐水平超过2.5 mg/dL这一旧标准,因此采用新定义时,与近期随机试验报告的结果相比,有可能使用特利加压素和白蛋白后HRS-AKI逆转的频率更高,且剂量更低或持续时间更短。然而,全身性炎症或基础肾实质损伤在多大程度上限制了HRS-AKI患者的治疗效果仍不清楚。进一步研发尿生物标志物并将其纳入诊断或治疗流程,有可能改善AKI的鉴别诊断、指导HRS-AKI的血管收缩药治疗,并协助预测肝移植后AKI的可逆性。需要通过进一步研究来确定预防和治疗AKI和HRS-AKI所需的白蛋白量,并支持床旁超声指导补液的更广泛应用。
作者信息
Mitra K. Nadim, M.D., and Guadalupe Garcia-Tsao, M.D.
From the Division of Nephrology and Hypertension, Keck School of Medicine, University of Southern California, Los Angeles (M.K.N.); and the Section of Digestive Diseases, Yale University School of Medicine, New Haven, and the Section of Digestive Diseases, Veterans Affairs Connecticut Healthcare System, West Haven — both in Connecticut (G.G.-T.). Dr. Garcia-Tsao can be contacted at guadalupe.garcia-tsao@yale.edu or at the Section of Digestive Diseases, Veterans Affairs Connecticut Healthcare System, 950 Campbell Ave., West Haven, CT 06516.
参考文献
- 1. Tandon P, James MT, Abraldes JG, Karvellas CJ, Ye F, Pannu N. Relevance of new definitions to incidence and prognosis of acute kidney injury in hospitalized patients with cirrhosis: a retrospective population-based cohort Study. PLoS One 2016;11(8):e0160394-e0160394.
- 2. Belcher JM, Garcia-Tsao G, Sanyal AJ, et al. Association of AKI with mortality and complications in hospitalized patients with cirrhosis. Hepatology 2013;57:753-762.
- 3. Garcia-Tsao G, Parikh CR, Viola A. Acute kidney injury in cirrhosis. Hepatology 2008;48:2064-2077.
- 4. Desai AP, Knapp SM, Orman ES, et al. Changing epidemiology and outcomes of acute kidney injury in hospitalized patients with cirrhosis — a US population-based study. J Hepatol 2020;73:1092-1099.
- 5. Amathieu R, Al-Khafaji A, Sileanu FE, et al. Significance of oliguria in critically ill patients with chronic liver disease. Hepatology 2017;66:1592-1600.
- 6. Nadim MK, Genyk YS, Tokin C, et al. Impact of the etiology of acute kidney injury on outcomes following liver transplantation: acute tubular necrosis versus hepatorenal syndrome. Liver Transpl 2012;18:539-548.
- 7. Salerno F, Gerbes A, Ginès P, Wong F, Arroyo V. Diagnosis, prevention and treatment of hepatorenal syndrome in cirrhosis. Gut 2007;56:1310-1318.
- 8. Nadim MK, Kellum JA, Davenport A, et al. Hepatorenal syndrome: the 8th International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care 2012;16(1):R23-R23.
- 9. Angeli P, Ginès P, Wong F, et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. J Hepatol 2015;62:968-974.
- 10. Angeli P, Garcia-Tsao G, Nadim MK, Parikh CR. News in pathophysiology, definition and classification of hepatorenal syndrome: a step beyond the International Club of Ascites (ICA) consensus document. J Hepatol 2019;71:811-822.
- 11. Ronco C, Bellomo R, Kellum JA. Acute kidney injury. Lancet 2019;394:1949-1964.
- 12. Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl 2012;2:1-138.
- 13. Nadim MK, Durand F, Kellum JA, et al. Management of the critically ill patient with cirrhosis: a multidisciplinary perspective. J Hepatol 2016;64:717-735.
- 14. Francoz C, Durand F, Kahn JA, Genyk YS, Nadim MK. Hepatorenal syndrome. Clin J Am Soc Nephrol 2019;14:774-781.
- 15. Schrier RW, Arroyo V, Bernardi M, Epstein M, Henriksen JH, Rodés J. Peripheral arterial vasodilation hypothesis: a proposal for the initiation of renal sodium and water retention in cirrhosis. Hepatology 1988;8:1151-1157.
- 16. Traykova D, Schneider B, Chojkier M, Buck M. Blood microbiome quantity and the hyperdynamic circulation in decompensated cirrhotic patients. PLoS One 2017;12(2):e0169310-e0169310.
- 17. Wiest R, Das S, Cadelina G, Garcia-Tsao G, Milstien S, Groszmann RJ. Bacterial translocation in cirrhotic rats stimulates eNOS-derived NO production and impairs mesenteric vascular contractility. J Clin Invest 1999;104:1223-1233.
- 18. Turco L, Garcia-Tsao G, Magnani I, et al. Cardiopulmonary hemodynamics and C-reactive protein as prognostic indicators in compensated and decompensated cirrhosis. J Hepatol 2018;68:949-958.
- 19. Danielsen KV, Wiese S, Busk T, et al. Cardiovascular mapping in cirrhosis from the compensated stage to hepatorenal syndrome: a magnetic resonance study. Am J Gastroenterol 2022;117:1269-1278.
- 20. Ruiz-del-Arbol L, Monescillo A, Arocena C, et al. Circulatory function and hepatorenal syndrome in cirrhosis. Hepatology 2005;42:439-447.
- 21. Macedo E, Bouchard J, Soroko SH, et al. Fluid accumulation, recognition and staging of acute kidney injury in critically-ill patients. Crit Care 2010;14(3):R82-R82.
- 22. Liu KD, Thompson BT, Ancukiewicz M, et al. Acute kidney injury in patients with acute lung injury: impact of fluid accumulation on classification of acute kidney injury and associated outcomes. Crit Care Med 2011;39:2665-2671.
- 23. Singapura P, Ma T-W, Sarmast N, et al. Estimating glomerular filtration rate in cirrhosis using creatinine-based and cystatin C-based equations: systematic review and meta-analysis. Liver Transpl 2021;27:1538-1552.
- 24. Asrani SK, Jennings LW, Trotter JF, et al. A model for glomerular filtration rate assessment in liver disease (GRAIL) in the presence of renal dysfunction. Hepatology 2019;69:1219-1230.
- 25. Asrani SK, Jennings LW, Kim WR, et al. MELD-GRAIL-Na: glomerular filtration rate and mortality on liver-transplant waiting list. Hepatology 2020;71:1766-1774.
- 26. Delgado C, Baweja M, Crews DC, et al. A unifying approach for GFR estimation: recommendations of the NKF-ASN Task Force on Reassessing the Inclusion of Race in Diagnosing Kidney Disease. Am J Kidney Dis 2022;79(2):268-288.
- 27. Panchal S, Serper M, Bittermann T, Asrani SK, Goldberg DS, Mahmud N. Impact of race-adjusted glomerular filtration rate estimation on eligibility for simultaneous liver-kidney transplantation. Liver Transpl 2022;28:959-968.
- 28. Belcher JM, Sanyal AJ, Peixoto AJ, et al. Kidney biomarkers and differential diagnosis of patients with cirrhosis and acute kidney injury. Hepatology 2014;60:622-632.
- 29. Alsaad AA, Wadei HM. Fractional excretion of sodium in hepatorenal syndrome: clinical and pathological correlation. World J Hepatol 2016;8:1497-1501.
- 30. Patidar KR, Kang L, Bajaj JS, Carl D, Sanyal AJ. Fractional excretion of urea: a simple tool for the differential diagnosis of acute kidney injury in cirrhosis. Hepatology 2018;68:224-233.
- 31. Huelin P, Solà E, Elia C, et al. Neutrophil gelatinase-associated lipocalin for assessment of acute kidney injury in cirrhosis: a prospective study. Hepatology 2019;70:319-333.
- 32. Asrani SK, Shankar N, da Graca B, Nadim MK, Cardenas A. Role of novel kidney biomarkers in patients with cirrhosis and after liver transplantation. Liver Transpl 2022;28:466-482.
- 33. Allegretti AS, Parada XV, Endres P, et al. Urinary NGAL as a diagnostic and prognostic marker for acute kidney injury in cirrhosis: a prospective study. Clin Transl Gastroenterol 2021;12(5):e00359-e00359.
- 34. Francoz C, Nadim MK, Durand F. Kidney biomarkers in cirrhosis. J Hepatol 2016;65:809-824.
- 35. Velez JCQ, Petkovich B, Karakala N, Huggins JT. Point-of-care echocardiography unveils misclassification of acute kidney injury as hepatorenal syndrome. Am J Nephrol 2019;50:204-211.
- 36. Ruiz-del-Arbol L, Monescillo A, Jimenéz W, Garcia-Plaza A, Arroyo V, Rodés J. Paracentesis-induced circulatory dysfunction: mechanism and effect on hepatic hemodynamics in cirrhosis. Gastroenterology 1997;113:579-586.
- 37. Biggins SW, Angeli P, Garcia-Tsao G, et al. Diagnosis, evaluation, and management of ascites, spontaneous bacterial peritonitis and hepatorenal syndrome: 2021 practice guidance by the American Association for the Study of Liver Diseases. Hepatology 2021;74:1014-1048.
- 38. European Association for the Study of the Liver. EASL clinical practice guidelines for the management of patients with decompensated cirrhosis. J Hepatol 2018;69:406-460.
- 39. Pitre T, Kiflen M, Helmeczi W, et al. The comparative effectiveness of vasoactive treatments for hepatorenal syndrome: a systematic review and network meta-analysis. Crit Care Med 2022;50:1419-1429.
- 40. Mohamed MMG, Rauf A, Adam A, Kheiri B, Lacasse A, El-Halawany H. Terlipressin effect on hepatorenal syndrome: updated meta-analysis of randomized controlled trials. JGH Open 2021;5:896-901.
- 41. Velez JC, Nietert PJ. Therapeutic response to vasoconstrictors in hepatorenal syndrome parallels increase in mean arterial pressure: a pooled analysis of clinical trials. Am J Kidney Dis 2011;58:928-938.
- 42. Cavallin M, Piano S, Romano A, et al. Terlipressin given by continuous intravenous infusion versus intravenous boluses in the treatment of hepatorenal syndrome: a randomized controlled study. Hepatology 2016;63:983-992.
- 43. Wong F, Pappas SC, Curry MP, et al. Terlipressin plus albumin for the treatment of type 1 hepatorenal syndrome. N Engl J Med 2021;384:818-828.
- 44. Cavallin M, Kamath PS, Merli M, et al. Terlipressin plus albumin versus midodrine and octreotide plus albumin in the treatment of hepatorenal syndrome: a randomized trial. Hepatology 2015;62:567-574.
- 45. Charilaou P, Devani K, Petrosyan R, Reddy C, Pyrsopoulos N. Inpatient mortality benefit with transjugular intrahepatic portosystemic shunt for hospitalized hepatorenal syndrome patients. Dig Dis Sci 2020;65:3378-3388.
- 46. Ponzo P, Campion D, Rizzo M, et al. Transjugular intrahepatic porto-systemic shunt in cirrhotic patients with hepatorenal syndrome — chronic kidney disease: impact on renal function. Dig Liver Dis 2022;54:1101-1108.
- 47. Boike JR, Thornburg BG, Asrani SK, et al. North American practice-based recommendations for transjugular intrahepatic portosystemic shunts in portal hypertension. Clin Gastroenterol Hepatol 2022;20(8):1636.e36-1662.e36.
- 48. Allegretti AS, Ortiz G, Cui J, et al. Changes in kidney function after transjugular intrahepatic portosystemic shunts versus large-volume paracentesis in cirrhosis: a matched cohort analysis. Am J Kidney Dis 2016;68:381-391.
- 49. Song T, Rössle M, He F, Liu F, Guo X, Qi X. Transjugular intrahepatic portosystemic shunt for hepatorenal syndrome: a systematic review and meta-analysis. Dig Liver Dis 2018;50:323-330.
- 50. Martín-Llahí M, Guevara M, Torre A, et al. Prognostic importance of the cause of renal failure in patients with cirrhosis. Gastroenterology 2011;140(2):488.e4-496.e4.
- 51. Allegretti AS, Parada XV, Eneanya ND, et al. Prognosis of patients with cirrhosis and aki who initiate RRT. Clin J Am Soc Nephrol 2018;13:16-25.
- 52. Zarbock A, Kellum JA, Schmidt C, et al. Effect of early vs delayed initiation of renal replacement therapy on mortality in critically ill patients with acute kidney injury: the ELAIN randomized clinical trial. JAMA 2016;315:2190-2199.
- 53. Gaudry S, Hajage D, Schortgen F, et al. Initiation strategies for renal-replacement therapy in the intensive care unit. N Engl J Med 2016;375:122-133.
- 54. Barbar SD, Clere-Jehl R, Bourredjem A, et al. Timing of renal-replacement therapy in patients with acute kidney injury and sepsis. N Engl J Med 2018;379:1431-1442.
- 55. Wald R, Bagshaw SM. Timing of initiation of renal-replacement therapy in acute kidney injury. N Engl J Med 2020;383:1797-1798.
- 56. Rosner MH, Ostermann M, Murugan R, et al. Indications and management of mechanical fluid removal in critical illness. Br J Anaesth 2014;113:764-771.
- 57. Bouchard J, Mehta RL. Timing of kidney support therapy in acute kidney injury: what are we waiting for? Am J Kidney Dis 2022;79:417-426.
- 58. Levitsky J, Baker T, Ahya SN, et al. Outcomes and native renal recovery following simultaneous liver-kidney transplantation. Am J Transplant 2012;12:2949-2957.
- 59. Nadim MK, Sung RS, Davis CL, et al. Simultaneous liver-kidney transplantation summit: current state and future directions. Am J Transplant 2012;12:2901-2908.
- 60. Formica RN, Aeder M, Boyle G, et al. Simultaneous liver-kidney allocation policy: a proposal to optimize appropriate utilization of scarce resources. Am J Transplant 2016;16:758-766.
- 61. Pichler RH, Huskey J, Kowalewska J, et al. Kidney biopsies may help predict renal function after liver transplantation. Transplantation 2016;100:2122-2128.
- 62. Levitsky J, Asrani SK, Klintmalm G, et al. Discovery and validation of a biomarker model (PRESERVE) predictive of renal outcomes after liver transplantation. Hepatology 2020;71:1775-1786.
- 63. Levitsky J, Asrani SK, Abecassis M, Ruiz R, Jennings LW, Klintmalm G. External validation of a pretransplant biomarker model (REVERSE) predictive of renal recovery after liver transplantation. Hepatology 2019;70:1349-1359.
- 64. O’Leary JGO, Levitsky J, Wong F, Nadim MK, Charlton M, Kim WR. Protecting the kidney in liver transplant candidates: practice-based recommendations from the American Society of Transplantation Liver and Intestine Community of Practice. Am J Transplant 2016;16:2516-2531.
- 65. de Franchis R, Bosch J, Garcia-Tsao G, Reiberger T, Ripoll C. Baveno VII — renewing consensus in portal hypertension. J Hepatol 2022;76:959-974.
- 66. Bernardi M, Caraceni P, Navickis RJ, Wilkes MM. Albumin infusion in patients undergoing large-volume paracentesis: a meta-analysis of randomized trials. Hepatology 2012;55:1172-1181.
- 67. Sort P, Navasa M, Arroyo V, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. N Engl J Med 1999;341:403-409.
- 68. Thévenot T, Bureau C, Oberti F, et al. Effect of albumin in cirrhotic patients with infection other than spontaneous bacterial peritonitis: a randomized trial. J Hepatol 2015;62:822-830.
- 69. Caraceni P, Riggio O, Angeli P, et al. Long-term albumin administration in decompensated cirrhosis (ANSWER): an open-label randomised trial. Lancet 2018;391:2417-2429.
- 70. Solà E, Solé C, Simón-Talero M, et al. Midodrine and albumin for prevention of complications in patients with cirrhosis awaiting liver transplantation: a randomized placebo-controlled trial. J Hepatol 2018;69:1250-1259.
- 71. China L, Freemantle N, Forrest E, et al. A randomized trial of albumin infusions in hospitalized patients with cirrhosis. N Engl J Med 2021;384:808-817.
- 72. Davenport MS, Perazella MA, Yee J, et al. Use of intravenous iodinated contrast media in patients with kidney disease: consensus statements from the American College of Radiology and the National Kidney Foundation. Kidney Med 2020;2:85-93.
特别申明:本文为转载文章,转载自NEJM医学前沿,不代表贪吃的夜猫子立场,如若转载,请注明出处:https://www.nejmqianyan.cn/article-info?permalinks=YXQYra2215289
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫