毒性醇包括甲醇、乙二醇、异丙醇、二甘醇和丙二醇等,醇中毒会引起细胞功能障碍和死亡1,但症状并无特异性。诊断延误会增加器官不可逆损伤和死亡的风险2。在这篇综述中,我们将讨论醇中毒的机制、诊断方法以及目前的治疗建议。
醇中毒的机制
毒性醇会引起迷醉,但除异丙醇外,其他醇并没有直接毒性,其毒性效应是由代谢物引起。图1A简要描绘了这几种醇的主要代谢途径。
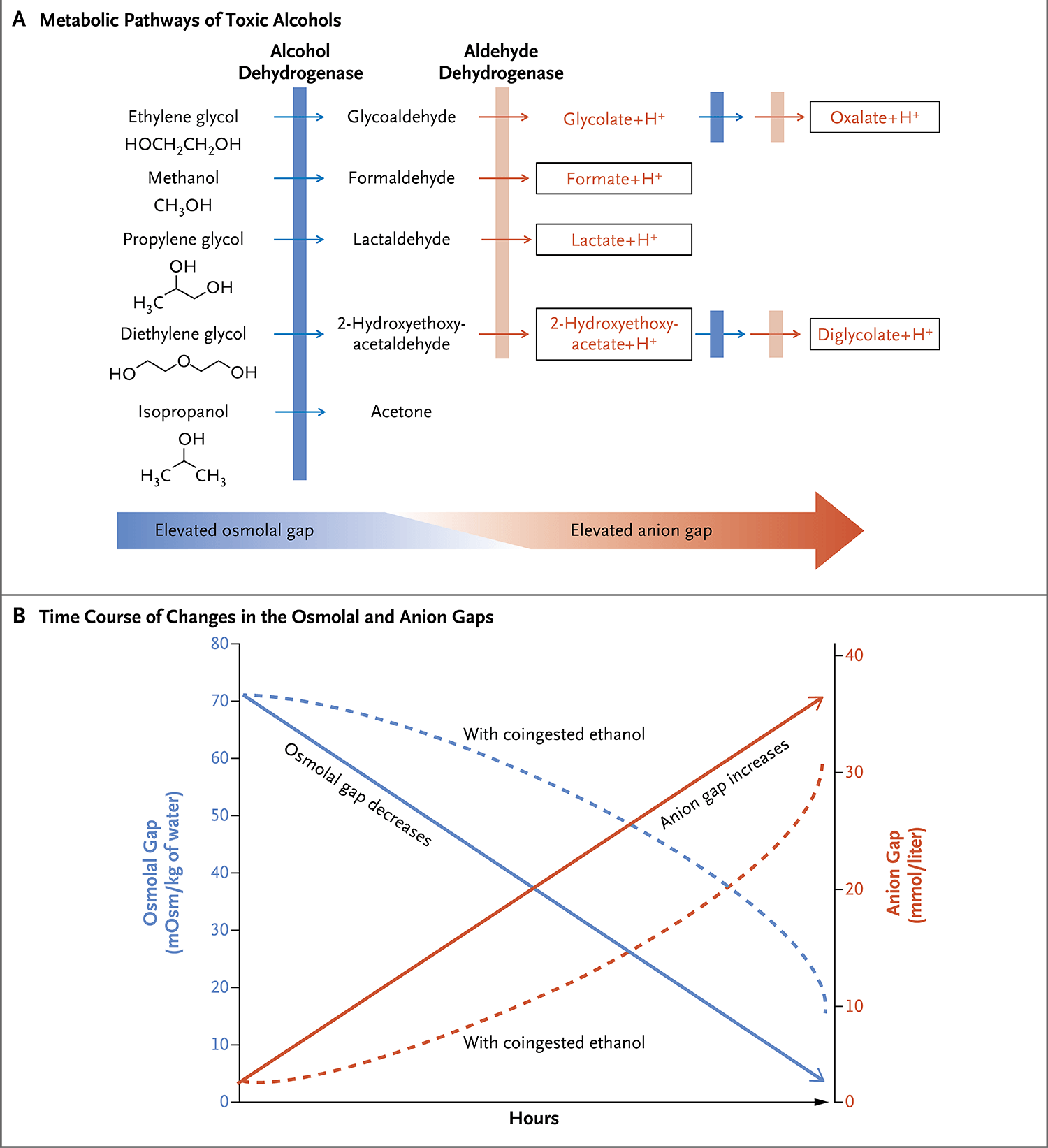
图A显示了毒性醇的代谢途径。醇脱氢酶和醛脱氢酶依次氧化毒性醇及其代谢物。毒性醇的首次氧化由醇脱氢酶催化完成,该过程是解毒治疗的重要目标。加框突出显示了推定的毒性代谢物。甲醇代谢为甲酸,乙二醇代谢为草酸和甘醇酸,二甘醇代谢为2-羟基乙氧基乙酸和羟基乙酸,丙二醇则代谢为D-乳酸和L-乳酸。图B显示了合并和不合并乙醇摄入的情况下,渗透压间隙和阴离子间隙随时间的变化。由于非离子化醇的蓄积,早期渗透压间隙增加较为明显。随着代谢进行,渗透压间隙随离子化代谢物的形成而下降。相反,在醇代谢之前,血清阴离子间隙处于最低值,而后会随着离子化代谢物的形成而升高。对于不同的醇,这两种参数随时间的变化是不同的。通常情况下,它们会在几小时至1天内逐渐变化。合并乙醇摄入会阻碍代谢(如虚线所示)并延迟高阴离子间隙酸中毒的发生。
毒性醇的第一次氧化经由醇脱氢酶催化进行,产生的醛(异丙醇氧化产生的丙酮除外)经醛脱氢酶催化进一步氧化形成羧酸代谢物:甲醇代谢为甲酸3,乙二醇代谢为草酸和甘醇酸3,二甘醇代谢为2-羟基乙氧基乙酸和羟基乙酸4,丙二醇则代谢为D-乳酸和L-乳酸5。醇脱氢酶是控制毒性代谢物产生的关键酶。同时摄入的乙醇是醇脱氢酶的竞争性底物,会延迟毒性代谢物的产生6。暴露于甲醇或乙二醇的代谢物可导致乳酸生成增多3,7,但暴露于乙二醇代谢物时,血液乳酸水平可能会出现假性升高,这是由于甘醇酸酯会干扰床边乳酸测量工具的准确性。
流行病学特征
中毒事件可经由不同途径发生(表1)。甲醇中毒最常见于摄入汽车挡风玻璃清洗液、工业用品或掺假酒品9,也可经肺部和皮肤途径中毒10。乙二醇中毒最常见于成人自杀性摄入汽车防冻剂或掺假烈酒(用乙二醇代替乙醇);儿童多为意外摄入。异丙醇中毒通常是由外用酒精、洗手液及各种工业用品摄入导致,但吸入或者经皮肤或直肠途径暴露也会中毒11。
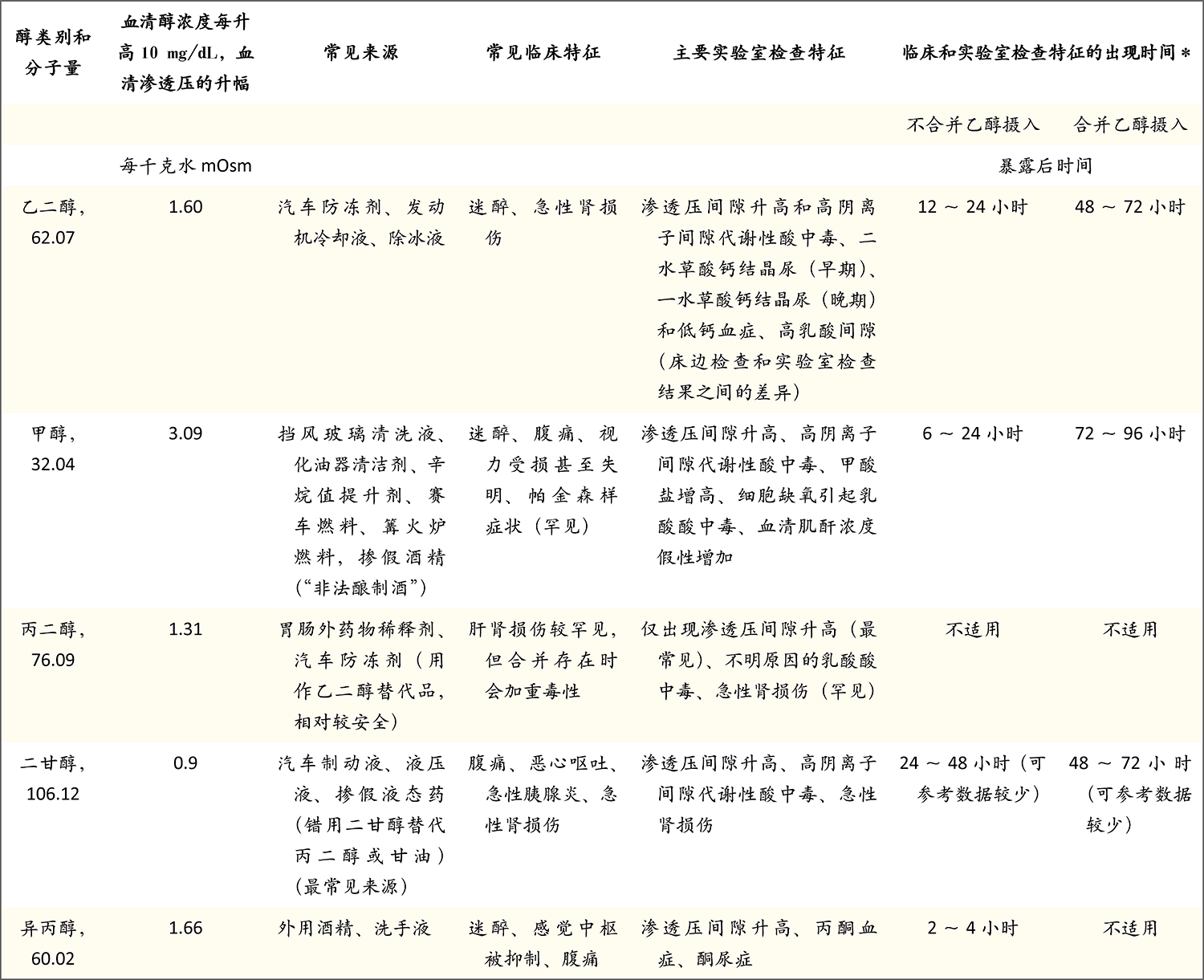
*不合并或合并乙醇摄入表示醇中毒患者同时存在乙醇的影响。NA表示不适用。
二甘醇中毒常由汽车制动液或工业用品摄入引起,但通常见于消费品或儿童口服药物使用二甘醇代替丙二醇作为稀释剂造成的中毒事件暴发12,13。极少数情况下,二甘醇经创伤皮肤吸收可产生毒性12-14。丙二醇存在于许多消费品和汽车防冻剂中,但中毒通常是由于长时间大剂量输注以丙二醇作为稀释剂的劳拉西泮等药物所致。
临床表现
暴露于毒性醇后,感觉中枢首先被抑制,而后器官出现功能障碍。甲醇与视力受损(见于29%~72%的病例16,偶尔会导致失明)、肺功能障碍、腹痛和昏迷相关,较少情况下还与帕金森样症状相关17。临床表现通常在6~24小时内逐步出现,但如果同时摄入乙醇,则可能会延迟至72~96小时出现18。暴露后数天或数周内可能出现神经系统后遗症19。
乙二醇中毒会形成草酸盐晶体,沉积在肺部、心脏和肾脏,并导致器官功能障碍20,21。颅神经损伤也有可能出现,不过有时会延迟数天出现。一般情况下,乙二醇暴露后,12小时内会出现神经功能障碍,12~24小时会出现心脏和肺功能障碍,48~72小时则会出现急性肾损伤22。不过,这些器官功能障碍也可能同步发生。暴露于乙二醇时,若同时摄入乙醇,临床异常会延迟出现20,22。
异丙醇中毒会抑制感觉中枢,并可能引起呼吸功能障碍、心血管衰竭、急性胰腺炎、低血压和乳酸酸中毒。血清异丙醇水平高于50 mg/dL(8.3 mmol/L)会出现明显临床表现,而血清水平高于150 mg/dL(25 mmol/L)则会导致深度昏迷23。需注意的是,丙酮会导致血清肌酐浓度假性增加,干扰实验室检查11。
二甘醇中毒可导致腹痛、恶心、呕吐、腹泻、急性胰腺炎、精神状态改变、肝脏疾病、中枢和周围神经病变(有时可导致四肢瘫痪)和急性肾损伤14。急性肾损伤通常在暴露后8~24小时出现,可能需要透析治疗,而且是主要致死原因24,25。暴露于二甘醇时,若同时摄入乙醇,中毒症状可延迟至48~72小时出现14。颅神经麻痹和其他神经系统并发症可能会在暴露后5天或更久时出现。
丙二醇中毒通常仅导致渗透压间隙(由冰点下降测得的血清渗透压与据下文等式算得的血清渗透压之差)增大22,23,但乳酸酸中毒和急性肾损伤也有可能出现。既有的肝脏疾病和(或)肾脏疾病都是乳酸酸中毒和急性肾损伤的易感因素。持续输注大剂量劳拉西泮(> 10 mg/h)48小时以上的患者,丙二醇中毒的风险较高。
诊断
病史、体格检查、血液生化以及鉴定原型醇或其代谢物的检查有助于诊断。毒性醇的暴露史非常重要,因为不同醇中毒的临床症状并不具有特异性,而且临床症状表现与醇暴露之间还可能存在时间延迟。
血液化学谱
毒性醇在人体内的蓄积会增加血清渗透压和渗透压间隙。之后,有机酸阴离子的蓄积会增多血清阴离子间隙。血清渗透压可通过许多公式估算,但临床上可接受的公式如下:估算血清渗透压=(2×Na+[mmol/L])+(血液尿素氮[mg/dL]÷2.8)+(葡萄糖[mg/dL]÷18)。
正常渗透压间隙预期为每千克水10~20 mmol 26。渗透压间隙较高反映有渗透活性物质(如毒性醇)的蓄积。血清渗透压间隙的增幅取决于醇的血清浓度和分子量(表1)。
基础血清渗透压间隙可能小于每千克水10 mOsm甚至为负数27。如果患者基础渗透压间隙水平较低,毒性醇蓄积引起的水平增加则有可能被掩盖。渗透压间隙正常并不能排除毒性醇的摄入;有研究发现,一些醇中毒的患者渗透压间隙在正常范围内。
渗透压间隙在中毒过程中会发生变化(图1B)29,30。起初,原型醇的蓄积会使渗透压间隙增大,但随着代谢的进行,渗透压间隙会减小。同时摄入乙醇(见于10%~60%的甲醇和乙二醇中毒)31,32会导致渗透压间隙进一步增加(血清醇浓度每增加10 mg/dL,渗透压间隙会增加每千克水2.17 mOsm),毒性醇代谢也会减缓,使渗透压间隙高水平状态的持续时间延长4。
血清阴离子间隙的基线值(即由醇代谢产生的有机酸阴离子蓄积之前)最高值和最低值之间的差值可达10 mmol/L 33。如果基线阴离子间隙水平较低,即便有机酸阴离子大量蓄积,也有可能不超过正常上限33,34。此外,随着毒性醇逐步代谢,阴离子间隙也会增加(图1B)。中毒患者可能表现为渗透压间隙正常或较高,血清阴离子间隙正常或偏高20,28,30,35。
渗透压间隙或阴离子间隙水平升高不一定意味着醇中毒。乳酸酸中毒、酮症酸中毒、慢性肾疾病和病细胞综合征都可能使其水平升高36。一项研究发现,渗透压和阴离子间隙增加的患者中仅有少数为醇中毒28。一些含甲醇和硝基甲烷的赛车燃料,通过雅费氏反应(Jaffe reaction)干扰实验室检查,使肌酐浓度假性升高37,38。
乙二醇代谢为草酸,导致结晶尿,甚至重度急性肾损伤20,39。二水合物晶体出现较早,一水合物晶体出现较晚。草酸盐与钙共沉淀偶尔会产生低钙血症20,40。异丙醇代谢产生的丙酮可产生高浓度乙酰乙酸盐的阳性硝普钠反应11。由于L-异构体的蓄积,乳酸酸中毒在丙烯中毒中最为常见,但有些情况下,D-乳酸酸中毒也会发生41。通常,乳酸酸中毒检测方法仅评估L-异构体乳酸水平,并不能发现D-乳酸酸中毒,从而导致漏诊。
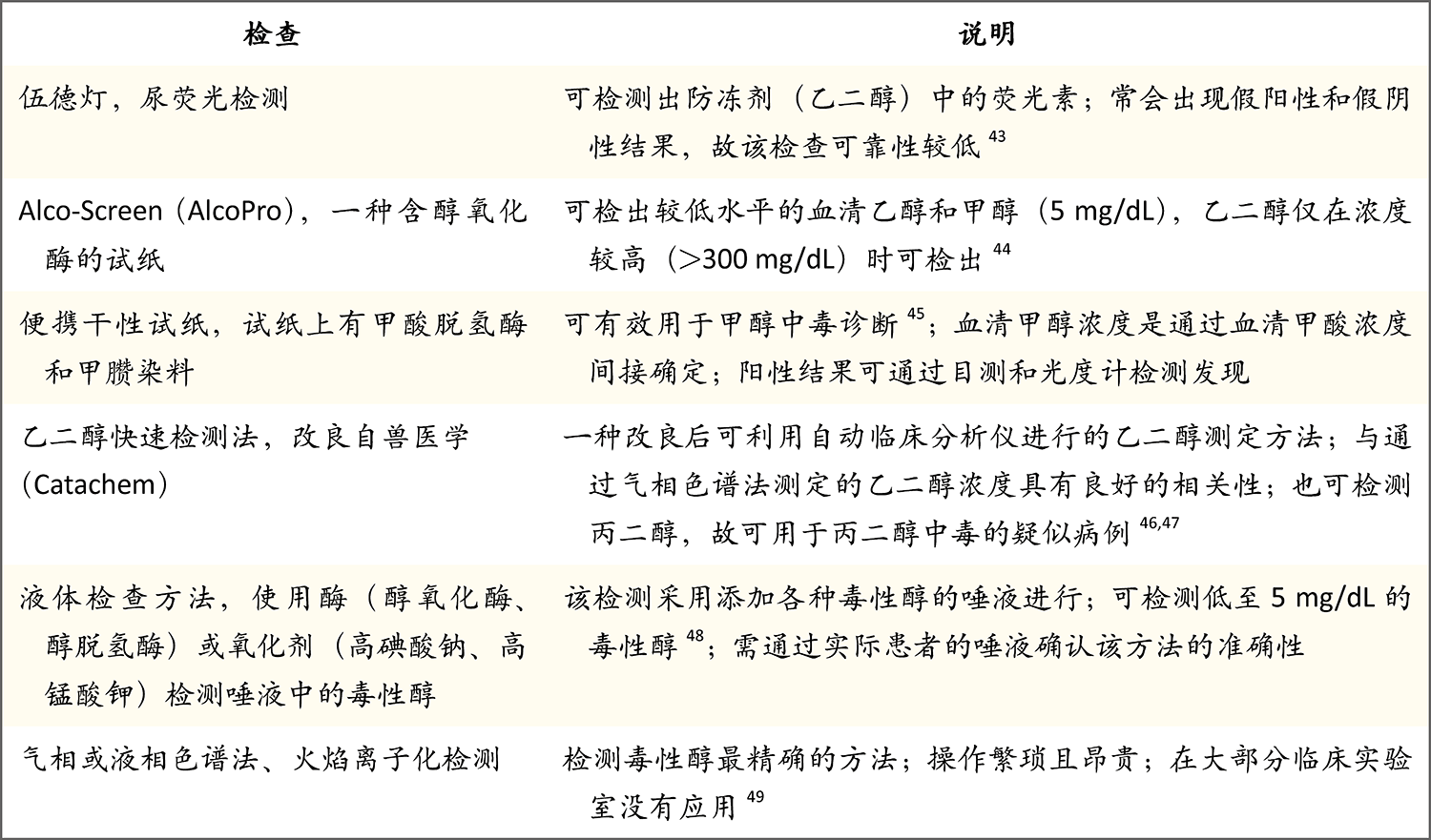
气相色谱法或液相色谱法可最准确鉴别体液中的毒性醇,并为其定量,但操作相对繁琐,价格昂贵,且并未广泛应用42。表2列出了目前正在使用或研发中的毒性醇鉴定方法27,43,46-48,50。实验室数据解读的常见错误有未注意浓度可能以mg/L或mg/dL表示,而数值高于200 mg/L或20 mg/dL表示需要治疗。此外,挥发性物质检查可能会鉴定出甲醇、乙醇、丙酮和异丙醇,但并不能鉴定乙二醇或二甘醇。
* 将乙醇、甲醇和乙二醇的数值转换成以mmol/L为单位时,乙醇乘以0.2171,甲醇乘以0.3121,乙二醇乘以0.1611。
治疗
醇中毒治疗延误会导致结局变差51。因此,当强烈怀疑有醇中毒或存在原因不明的代谢性酸中毒时,应立即开始治疗52。目前,针对醇中毒的诊断和治疗,不同专家的方法可能存在差异,而我们根据自身经验和当前文献,也绘制了一张诊治流程图,见图2。

该流程图提供了三种最常见醇中毒的诊断和治疗方法。二甘醇中毒较为罕见,但类似方法也可能有效。透析操作中,解毒剂给药后血清乙二醇浓度>300 mg/mL这一标准来自本文第二作者的临床实践。将甲醇、乙二醇和异丙醇的值转换为以mmol/L为单位时,甲醇乘以0.3121,乙二醇乘以0.1611,异丙醇乘以0.1664。
甲醇和乙二醇
甲醇或乙二醇的胃肠吸收快,所以胃净化(gastric decontamination)通常并无帮助。治疗包括阻止代谢,并从体内清除醇及其代谢物10,51,53-55。
静脉给予碱溶液可纠正代谢性酸中毒,并增加甲酸盐的电离作用,促进其经尿液排泄,同时减少其进入视神经56。血清甲醇或乙二醇水平高于20 mg/dL(甲醇,6 mmol/L;乙二醇,3 mmol/L),且患者具有明确的醇摄入病史,或强烈怀疑摄入有某种醇且渗透压间隙大于每千克水10 mOsm或有原因不明的代谢性酸中毒时,应开始解毒治疗(美国临床毒理学学会[American Academy of Clinical Toxicology, AACT]指南推荐;见补充附录1表S1。该表与本文全文一起,可在NEJM.org获取)。乙醇与醇脱氢酶的亲和力非常高,故常用静脉注射乙醇进行治疗57,不过该方法并未获得美国食品药品管理局(FDA)批准。血清乙醇浓度为100 mg/dL(22 mmol/L)可对酶产生竞争性抑制作用。其优点包括容易获取、价格低廉。缺点包括,静脉注射用药需由药剂师配制,需要频繁监测血清浓度,其对感觉中枢有抑制作用,且需在重症监护病房进行治疗。
甲吡唑(4-甲基吡唑)是醇脱氢酶的一种强效抑制剂(对醇脱氢酶的亲和力为乙醇的8,000倍),FDA分别在1997年和2000年批准其用于治疗乙二醇和甲醇中毒52,但并未批准用于其他醇中毒的治疗。甲吡唑在较低血药浓度时即有效,副作用小,且无须在重症监护条件下用药58,59。对于未接受透析治疗的患者,负荷剂量为15 mg/kg,此后每12小时给予维持剂量10 mg/kg 52。48小时后,维持剂量增至每12小时15 mg/kg,这是由于甲吡唑可通过细胞色素P-450酶系统诱导其自身的代谢。甲吡唑可经透析清除,因此推荐在透析后立即给药。更具体的给药时间可见药品说明书(补充附录1)60。
在美国,甲吡唑常用来治疗甲醇和乙二醇中毒。在2012年和2015年,90%~94%的患者使用甲吡唑进行治疗,5%~6%使用了乙醇61。美国以外地区,甲吡唑应用尚不广泛,乙醇的使用率更高55,62。无静脉注射乙醇可用时,口服乙醇也有治疗效果64。2013年,世界卫生组织将甲吡唑列入基本药物标准清单65。
对1974年至2010年8月的文献进行的一项系统综述显示,摄入甲醇或乙二醇后经乙醇治疗的患者,死亡率分别为21.8%和18.1%59;经甲吡唑治疗的患者死亡率分别为17.1%和4.1%。乙醇治疗中不良事件发生率高于甲吡唑(57% vs. 12%)66。甲吡唑的费用通常是弃用的原因,不过仿制药的引入已使花费大幅降低58。因此,甲吡唑是治疗此类中毒的首选药物;甲吡唑不可用时,乙醇也可有效治疗63,67。
毒性醇及其代谢物分子均较小,且为水溶性,可在血液透析过程中清除。补充附录1表S1提供了AACT使用血液透析治疗甲醇51或乙二醇53中毒的指南,以及中毒体外治疗工作组(Extracorporeal Treatments in Poisoning Workgroup, EXTRIP)35使用透析治疗甲醇中毒的指南。一般而言,对于重度代谢性酸中毒、血清甲醇和乙二醇浓度高于50 mg/dL(甲醇,16 mmol/L;乙二醇,8 mmol/L),支持治疗后生命体征仍恶化、有视力问题(甲醇中毒)或急性肾损伤的情况,两种指南均推荐透析。间歇性血液透析(使用大表面积透析器和高通量透析膜)比连续性肾脏替代疗法可更快地清除毒性醇35,68,69。
已有报告称,单独使用甲吡唑(未行血液透析)治疗甲醇或乙二醇中毒,无不良后果31,70-72。然而,这种情况下,甲醇和乙二醇的清除半衰期分别延长至71小时31和16小时58,联用透析时两者分别为2.5和2.7小时。暴露时间越长,住院天数和花费越多,这是一些专家支持血液透析的原因73。治疗的费用依赖于几个因素,包括毒性醇暴露量、药物的相对成本、透析和病房费用;进行治疗决策时应考虑这些因素74。
儿童的治疗与成人相似75。醇中毒治疗时,联合或不联合醇脱氢酶抑制剂的血液透析的价值和局限性有必要进行进一步评估。补充附录2(可在NEJM.org获取)中提供有一个交互式程序,可预测将原型醇和代谢物减少到安全水平所需的透析时间76。毒性醇和(或)其代谢物或在体内进行再分布,可能需要重复透析。
对于甲醇中毒患者,每4~6小时给予1 mg/kg叶酸可促进甲酸向二氧化碳和水转化。对于乙二醇中毒患者,吡哆醇(维生素B₆)和硫胺素(维生素B1)可促进甘醇酸代谢成毒性较低的化合物56。
二甘醇
对于二甘醇中毒,有专家建议使用醇脱氢酶抑制剂治疗58,72。单独使用甲吡唑成功治疗已有报告77,但因为二甘醇中毒患者常见急性肾损伤,所以使用甲吡唑联合血液透析治疗应该是合理的78。
异丙醇
对于异丙醇中毒,支持治疗通常足以逆转;但如果血清异丙醇浓度为500 mg/dL(83 mmol/L)或更高,或存在低血压或乳酸酸中毒,则可能必须进行血液透析11。醇脱氢酶抑制剂会减缓异丙醇的清除,应避免应用23。
丙二醇
大多数情况下,含有丙二醇的药物一经停用,较高水平的血清渗透压即会回落5。有关甲吡唑的应用尚未达成共识,但如果出现乳酸酸中毒,则建议进行血液透析5,79。
患者监护
重度中毒或血流动力学不稳定的患者,以及接受乙醇治疗的患者需在重症监护病房照护,而较轻度中毒或血流动力学稳定的患者,以及接受甲吡唑治疗的患者可在重症监护病房外进行安全照护。评估治疗反应时,有必要测量酸碱参数、电解质水平、肾功能和血清渗透压。毒性醇血清浓度的监测可最为理想地反映治疗效果,但通常并不能及时获得;这种情况下,可通过渗透压间隙来估计16,80。中毒治疗应持续至乙二醇或甲醇的血清浓度低于20~30 mg/dL(乙二醇,3~5 mmol/L;甲醇,6~9 mmol/L)21,35。
总结和展望
甲醇、乙二醇和二甘醇中毒,如未能及时识别、治疗,可导致严重的细胞功能障碍和高死亡率。异丙醇经常导致躯体类并发症,但死亡风险较低。高阴离子间隙代谢性酸中毒和(或)血清渗透压间隙升高都可提示血液中存在一种毒性醇,不过存在毒性醇时此类实验室异常结果不一定会出现。对于有前述临床表现的患者、所有反应迟钝的患者,或有不明原因的高渗透压间隙和(或)高阴离子间隙代谢性酸中毒的患者,应强烈怀疑存在某种醇中毒。即使在发达国家,高压液相色谱等确切的检查方法也未能广泛应用,不发达国家则尤为如此。因此,准确、快速检查的需求尚未得以满足。
醇脱氢酶抑制剂和透析法可有效治疗醇中毒,但某些情况下,患者并没有机会应用这两种治疗方法。此外,关于何时使用其中一种或两种方法尚无定论。对这些醇中毒反应的发病机制,我们目前已经有了更多的认识,并且找到了有效的治疗方法,但仍需做大量工作来消除醇暴露,进而消除暴露导致的严重临床症状。
作者信息
Jeffrey A. Kraut, M.D., and Michael E. Mullins, M.D.
From Medical and Research Services and Division of Nephrology, Veterans Health Administration Greater Los Angeles (VHAGLA) Healthcare System, and Membrane Biology Laboratory, David Geffen School of Medicine, University of California, Los Angeles — both in Los Angeles (J.A.K.); and the Division of Emergency Medicine, Washington University School of Medicine, St. Louis (M.E.M.). Address reprint requests to Dr. Kraut at the Division of Nephrology, VHAGLA Healthcare System, 11301 Wilshire Blvd., Bldg. 500, Rm. 6018, Los Angeles, CA 90073, or at jkraut@ucla.edu.
参考文献
- 1. Kraut JA, Kurtz I. Toxic alcohol ingestions: clinical features, diagnosis, and management. Clin J Am Soc Nephrol 2008;3:208-225
- 2. Mahieu P, Hassoun A, Lauwerys R. Predictors of methanol intoxication with unfavourable outcome. Hum Toxicol 1989;8:135-137
- 3. Jacobsen D, McMartin KE. Methanol and ethylene glycol poisonings: mechanism of toxicity, clinical course, diagnosis and treatment. Med Toxicol 1986;1:309-334
- 4. Robinson CN, Latimer B, Abreo F, Broussard K, McMartin KE. In-vivo evidence of nephrotoxicity and altered hepatic function in rats following administration of diglycolic acid, a metabolite of diethylene glycol. Clin Toxicol (Phila) 2017;55:196-205
- 5. Zar T, Graeber C, Perazella MA. Recognition, treatment, and prevention of propylene glycol toxicity. Semin Dial 2007;20:217-219
- 6. Ammar KA, Heckerling PS. Ethylene glycol poisoning with a normal anion gap caused by concurrent ethanol ingestion: importance of the osmolal gap. Am J Kidney Dis 1996;27:130-133
- 7. Latus J, Kimmel M, Alscher MD, Braun N. Ethylene glycol poisoning: a rare but life-threatening cause of metabolic acidosis — a single-centre experience. Clin Kidney J 2012;5:120-123
- 8. Verelst S, Vermeersch P, Desmet K. Ethylene glycol poisoning presenting with a falsely elevated lactate level. Clin Toxicol (Phila) 2009;47:236-238
- 9. Bennett IL Jr, Cary FH, Mitchell GL Jr, Cooper MN. Acute methyl alcohol poisoning: a review based on experiences in an outbreak of 323 cases. Medicine (Baltimore) 1953;32:431-463
- 10. Ghannoum M, Hoffman RS, Mowry JB, Lavergne V. Trends in toxic alcohol exposures in the United States from 2000 to 2013: a focus on the use of antidotes and extracorporeal treatments. Semin Dial 2014;27:395-401
- 11. Slaughter RJ, Mason RW, Beasley DM, Vale JA, Schep LJ. Isopropanol poisoning. Clin Toxicol (Phila) 2014;52:470-478
- 12. Cantarell MC, Fort J, Camps J, Sans M, Piera L, Rodamilans M. Acute intoxication due to topical application of diethylene glycol. Ann Intern Med 1987;106:478-479
- 13. Devoti E, Marta E, Belotti E, et al. Diethylene glycol poisoning from transcutaneous absorption. Am J Kidney Dis 2015;65:603-606
- 14. Schep LJ, Slaughter RJ, Temple WA, Beasley DM. Diethylene glycol poisoning. Clin Toxicol (Phila) 2009;47:525-535
- 15. Kapitein BS, Biesmans RS, van der Sijs HS, de Wildt SS. Propylene glycol-related delirium after esmolol infusion. Ann Pharmacother 2014;48:940-942
- 16. Hovda KE, Hunderi OH, Tafjord AB, Dunlop O, Rudberg N, Jacobsen D. Methanol outbreak in Norway 2002-2004: epidemiology, clinical features and prognostic signs. J Intern Med 2005;258:181-190
- 17. Karayel F, Turan AA, Sav A, Pakis I, Akyildiz EU, Ersoy G. Methanol intoxication: pathological changes of central nervous system (17 cases). Am J Forensic Med Pathol 2010;31:34-36
- 18. Haviv YS, Rubinger D, Zamir E, Safadi R. Pseudo-normal osmolal and anion gaps following simultaneous ethanol and methanol ingestion. Am J Nephrol 1998;18:436-438
- 19. Reddy NJ, Sudini M, Lewis LD. Delayed neurological sequelae from ethylene glycol, diethylene glycol and methanol poisonings. Clin Toxicol (Phila) 2010;48:967-973
- 20. Alhamad T, Blandon J, Meza AT, Bilbao JE, Hernandez GT. Acute kidney injury with oxalate deposition in a patient with a high anion gap metabolic acidosis and a normal osmolal gap. J Nephropathol 2013;2:139-143
- 21. McMartin K. Are calcium oxalate crystals involved in the mechanism of acute renal failure in ethylene glycol poisoning? Clin Toxicol (Phila) 2009;47:859-869
- 22. McQuade DJ, Dargan PI, Wood DM. Challenges in the diagnosis of ethylene glycol poisoning. Ann Clin Biochem 2014;51:167-178
- 23. Pappas AA, Ackerman BH, Olsen KM, Taylor EH. Isopropanol ingestion: a report of six episodes with isopropanol and acetone serum concentration time data. J Toxicol Clin Toxicol 1991;29:11-21
- 24. Sosa NR, Rodriguez GM, Schier JG, Sejvar JJ. Clinical, laboratory, diagnostic, and histopathologic features of diethylene glycol poisoning — Panama, 2006. Ann Emerg Med 2014;64:38-47
- 25. Landry GM, Martin S, McMartin KE. Diglycolic acid is the nephrotoxic metabolite in diethylene glycol poisoning inducing necrosis in human proximal tubule cells in vitro. Toxicol Sci 2011;124:35-44
- 26. Dorwart WV, Chalmers L. Comparison of methods for calculating serum osmolality form chemical concentrations, and the prognostic value of such calculations. Clin Chem 1975;21:190-194
- 27. Kraut JA. Diagnosis of toxic alcohols: limitations of present methods. Clin Toxicol (Phila) 2015;53:589-595
- 28. Krasowski MD, Wilcoxon RM, Miron J. A retrospective analysis of glycol and toxic alcohol ingestion: utility of anion and osmolal gaps. BMC Clin Pathol 2012;12:1-1
- 29. Hovda KE, Hunderi OH, Rudberg N, Froyshov S, Jacobsen D. Anion and osmolal gaps in the diagnosis of methanol poisoning: clinical study in 28 patients. Intensive Care Med 2004;30:1842-1846
- 30. Ku E, Cheung EL, Khan A, Yu ASL. Anion and osmolal gaps after alcohol intoxication. Am J Kidney Dis 2009;54:385-388
- 31. Hovda KE, Froyshov S, Gudmundsdottir H, Rudberg N, Jacobsen D. Fomepizole may change indication for hemodialysis in methanol poisoning: prospective study in seven cases. Clin Nephrol 2005;64:190-197
- 32. Brent J, McMartin K, Phillips S, et al. Fomepizole for the treatment of ethylene glycol poisoning. N Engl J Med 1999;340:832-838
- 33. Kraut JA, Nagami GT. The serum anion gap in the evaluation of acid-base disorders: what are its limitations and can its effectiveness be improved? Clin J Am Soc Nephrol 2013;8:2018-2024
- 34. Iberti TJ, Leibowitz AB, Papadakos PJ, Fischer EP. Low sensitivity of the anion gap as a screen to detect hyperlactatemia in critically ill patients. Crit Care Med 1990;18:275-277
- 35. Roberts DM, Yates C, Megarbane B, et al. Recommendations for the role of extracorporeal treatments in the management of acute methanol poisoning: a systematic review and consensus statement. Crit Care Med 2015;43:461-472
- 36. Kraut JA, Xing SX. Approach to the evaluation of a patient with an increased serum osmolal gap and high-anion-gap metabolic acidosis. Am J Kidney Dis 2011;58:480-484
- 37. Rastogi A, Itagaki B, Bajwa M, Kraut JA. Spurious elevation in serum creatinine caused by ingestion of nitromethane: implication for the diagnosis and treatment of methanol intoxication. Am J Kidney Dis 2008;52:181-187
- 38. Mullins ME, Hammett-Stabler CA. Intoxication with nitromethane-containing fuels: don’t be “fueled” by the creatinine. J Toxicol Clin Toxicol 1998;36:315-320
- 39. Guo C, Cenac TA, Li Y, McMartin KE. Calcium oxalate, and not other metabolites, is responsible for the renal toxicity of ethylene glycol. Toxicol Lett 2007;173:8-16
- 40. Hodgman M, Marraffa JM, Wojcik S, Grant W. Serum calcium concentration in ethylene glycol poisoning. J Med Toxicol 2017;13:153-157
- 41. Jorens PG, Demey HE, Schepens PJC, et al. Unusual D-lactic acid acidosis from propylene glycol metabolism in overdose. J Toxicol Clin Toxicol 2004;42:163-169
- 42. Van Hee P, Neels H, De Doncker M, et al. Analysis of gamma-hydroxybutyric acid, DL-lactic acid, glycolic acid, ethylene glycol and other glycols in body fluids by a direct injection gas chromatography-mass spectrometry assay for wide. Clin Chem Lab Med 2004;42:1341-1345
- 43. Parsa T, Cunningham SJ, Wall SP, Almo SC, Crain EF. The usefulness of urine fluorescence for suspected antifreeze ingestion in children. Am J Emerg Med 2005;23:787-792
- 44. Hack JB, Early J, Brewer KL. An alcohol oxidase dipstick rapidly detects methanol in the serum of mice. Acad Emerg Med 2007;14:1130-1134
- 45. Hovda KE, Urdal P, Jacobsen D. Increased serum formate in the diagnosis of methanol poisoning. J Anal Toxicol 2005;29:586-588
- 46. Juenke JM, Hardy L, McMillin GA, Horowitz GL. Rapid and specific quantification of ethylene glycol levels: adaptation of a commercial enzymatic assay to automated chemistry analyzers. Am J Clin Pathol 2011;136:318-324
- 47. Rooney SL, Ehlers A, Morris C, et al. Use of a rapid ethylene glycol assay: a 4-year retrospective study at an academic medical center. J Med Toxicol 2016;12:172-179
- 48. Shin JM, Sachs G, Kraut JA. Simple diagnostic tests to detect toxic alcohol intoxications. Transl Res 2008;152:194-201
- 49. Eder AF, McGrath CM, Dowdy YG, et al. Ethylene glycol poisoning: toxicokinetic and analytical factors affecting laboratory diagnosis. Clin Chem 1998;44:168-177
- 50. Casavant MJ, Shah MN, Battels R. Does fluorescent urine indicate antifreeze ingestion by children? Pediatrics 2001;107:113-114
- 51. Barceloux DG, Bond GR, Krenzelok EP, Cooper H, Vale JA. American Academy of Clinical Toxicology practice guidelines on the treatment of methanol poisoning. J Toxicol Clin Toxicol 2002;40:415-446
- 52. Brent J. Fomepizole for ethylene glycol and methanol poisoning. N Engl J Med 2009;360:2216-2223
- 53. Barceloux DG, Krenzelok EP, Olson K, Watson W. American Academy of Clinical Toxicology practice guidelines on the treatment of ethylene glycol poisoning. J Toxicol Clin Toxicol 1999;37:537-560
- 54. Abramson S, Singh AK. Treatment of the alcohol intoxications: ethylene glycol, methanol and isopropanol. Curr Opin Nephrol Hypertens 2000;9:695-701
- 55. Zakharov S, Pelclova D, Navratil T, et al. Fomepizole versus ethanol in the treatment of acute methanol poisoning: comparison of clinical effectiveness in a mass poisoning outbreak. Clin Toxicol (Phila) 2015;53:797-806
- 56. Jacobsen D, Webb R, Collins TD, McMartin KE. Methanol and formate kinetics in late diagnosed methanol intoxication. Med Toxicol Adverse Drug Exp 1988;3:418-423
- 57. Wacker WE, Haynes H, Druyan R, Fisher W, Coleman JE. Treatment of ethylene glycol poisoning with ethyl alcohol. JAMA 1965;194:1231-1233
- 58. McMartin K, Jacobsen D, Hovda KE. Antidotes for poisoning by alcohols that form toxic metabolites. Br J Clin Pharmacol 2016;81:505-515
- 59. Beatty L, Green R, Magee K, Zed P.. A systematic review of ethanol and fomepizole use in toxic alcohol ingestions. Emerg Med Int 2013;2013:638057-638057
- 60. Antizol (fomepizole): highlights of prescribing information. Montreal: Paladin Labs, 2009.
- 61. Mowry JB, Spyker DA, Brooks DE, Zimmerman A, Schauben JL. 2015 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 33rd Annual Report. Clin Toxicol (Phila) 2016;54:924-1109
- 62. Thanacoody RH, Gilfillan C, Bradberry SM, et al. Management of poisoning with ethylene glycol and methanol in the UK: a prospective study conducted by the National Poisons Information Service (NPIS). Clin Toxicol (Phila) 2016;54:134-140
- 63. Rietjens SJ, de Lange DW, Meulenbelt J. Ethylene glycol or methanol intoxication: which antidote should be used, fomepizole or ethanol? Neth J Med 2014;72:73-79
- 64. Zakharov S, Pelclova D, Urban P, et al. Use of out-of-hospital ethanol administration to improve outcome in mass methanol outbreaks. Ann Emerg Med 2016;68:52-61
- 65. WHO model list of essential medicines: 18th list. Geneva: World Health Organization, 2013.
- 66. Lepik KJ, Levy AR, Sobolev BG, et al. Adverse drug events associated with the antidotes for methanol and ethylene glycol poisoning: a comparison of ethanol and fomepizole. Ann Emerg Med 2009;53:439-450.e10
- 67. Anseeuw K, Sabbe MB, Legrand A. Methanol poisoning: the duality between ‘fast and cheap’ and ‘slow and expensive.’ Eur J Emerg Med 2008;15:107-109
- 68. Zakharov S, Pelclova D, Navratil T, et al. Intermittent hemodialysis is superior to continuous veno-venous hemodialysis/hemodiafiltration to eliminate methanol and formate during treatment for methanol poisoning. Kidney Int 2014;86:199-207
- 69. Peces R, Fernández R, Peces C, et al. Effectiveness of pre-emptive hemodialysis with high-flux membranes for the treatment of life-threatening alcohol poisoning Nefrologia 2008;28:413-418
- 70. Borron SW, Mégarbane B, Baud FJ. Fomepizole in treatment of uncomplicated ethylene glycol poisoning. Lancet 1999;354:831-831
- 71. Mégarbane B, Borron SW, Trout H, et al. Treatment of acute methanol poisoning with fomepizole. Intensive Care Med 2001;27:1370-1378
- 72. Mégarbane B, Borron SW, Baud FJ. Current recommendations for treatment of severe toxic alcohol poisonings. Intensive Care Med 2005;31:189-195
- 73. Hovda KE, Mundal H, Urdal P, McMartin K, Jacobsen D. Extremely slow formate elimination in severe methanol poisoning: a fatal case report. Clin Toxicol (Phila) 2007;45:516-521
- 74. Wiles D, Tzeng J, Russell J, Casavant MJ. Comment on treatment methods for ethylene glycol intoxication. Neth J Med 2014;72:383-384
- 75. Brent J. Fomepizole for the treatment of pediatric ethylene and diethylene glycol, butoxyethanol, and methanol poisonings. Clin Toxicol (Phila) 2010;48:401-406
- 76. Hirsch DJ, Jindal KK, Wong P, Fraser AD. A simple method to estimate the required dialysis time for cases of alcohol poisoning. Kidney Int 2001;60:2021-2024
- 77. Borron SW, Baud FJ, Garnier R. Intravenous 4-methylpyrazole as an antidote for diethylene glycol and triethylene glycol poisoning: a case report. Vet Hum Toxicol 1997;39:26-28
- 78. Brophy PD, Tenenbein M, Gardner J, Bunchman TE, Smoyer WE. Childhood diethylene glycol poisoning treated with alcohol dehydrogenase inhibitor fomepizole and hemodialysis. Am J Kidney Dis 2000;35:958-962
- 79. Pillai U, Hothi JC, Bhat ZY. Severe propylene glycol toxicity secondary to use of anti-epileptics. Am J Ther 2014;21:e106-e109
- 80. Hunderi OH, Hovda KE, Jacobsen D. Use of the osmolal gap to guide the start and duration of dialysis in methanol poisoning. Scand J Urol Nephrol 2006;40:70-74
特别申明:本文为转载文章,转载自NEJM医学前沿,不代表贪吃的夜猫子立场,如若转载,请注明出处:https://www.nejmqianyan.cn/article-info?permalinks=YXQYra1615295
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫