Abstract
Background: Severe protein catabolism is a major aspect of critical illness and leads to pronounced muscle wasting and, consequently, extended intensive care unit (ICU) stay and increased mortality. The urea-to-creatinine ratio (UCR) has emerged as a promising biomarker for assessing protein catabolism in critical illness, which is currently lacking. This review aims to elucidate the role of UCR in the context of critical illness.
严重的蛋白质分解代谢是危重症的主要特征之一,可导致显著的肌肉消耗,进而延长重症监护病房(ICU)住院时间并增加死亡率。尿素与肌酐比值(UCR)作为一种评估危重症患者蛋白质分解代谢的新兴生物标志物,目前尚缺乏系统性研究。本综述旨在阐明UCR在危重症背景下的作用。
Methods: This scoping review adhered to the PRISMA Extension for Scoping Reviews guidelines. A comprehensive literature search was conducted on the 3rd of September 2024, across Embase, PubMed, ScienceDirect, and Cochrane Library to identify studies related to (1) critically ill adult patients and (2) reporting at least a single UCR value. A meta-analysis was conducted for ≥ 5 studies with identical outcome parameters.
本范围综述遵循《PRISMA范围综述扩展指南》。于2024年9月3日对Embase、PubMed、ScienceDirect和Cochrane Library进行了全面的文献检索,筛选出符合以下标准的研究:(1)针对成年危重症患者;(2)报告了至少一个UCR值。对于结果参数相同的≥5项研究进行了荟萃分析。
Results: Out of 1,450 studies retrieved, 47 were included in this review, focusing on UCR’s relation to protein catabolism and persistent critical illness (10 studies), mortality (16 studies), dietary protein interventions (2 studies), and other outcomes (19 studies), such as delirium, and neurological and cardiac adverse events. UCR is inversely correlated to muscle cross-sectional area over time and associated to length of ICU stay, emphasising its potential role in identifying patients with ongoing protein catabolism. A UCR (BUN-to-creatinine in mg/dL) of ≥ 20 (equivalent to a urea-to-creatinine in mmol/L of approximately 80) upon ICU admission, in comparison with a value < 20, was associated with a relative risk of 1.60 (95% CI 1.27-2.00) and an adjusted hazard ratio of 1.29 (95% CI 0.89-1.86) for in-hospital mortality.
在检索到的1,450项研究中,有47项被纳入本综述。这些研究主要探讨了UCR与以下方面的关系:蛋白质分解代谢与持续性危重症(10项研究)、死亡率(16项研究)、膳食蛋白质干预(2项研究)以及其他结局指标(19项研究),如谵妄、神经系统和心脏不良事件。UCR与肌肉横截面积随时间呈负相关,并与ICU住院时间相关,这强调了其在识别持续蛋白质分解代谢患者中的潜在作用。在ICU入院时UCR(以BUN/肌酐,单位为mg/dL计)≥20(相当于以mmol/L计的尿素/肌酐约80)的患者,与UCR <20的患者相比,其住院死亡率的相对风险为1.60(95% CI 1.27-2.00),调整后的风险比为1.29(95% CI 0.89-1.86)。
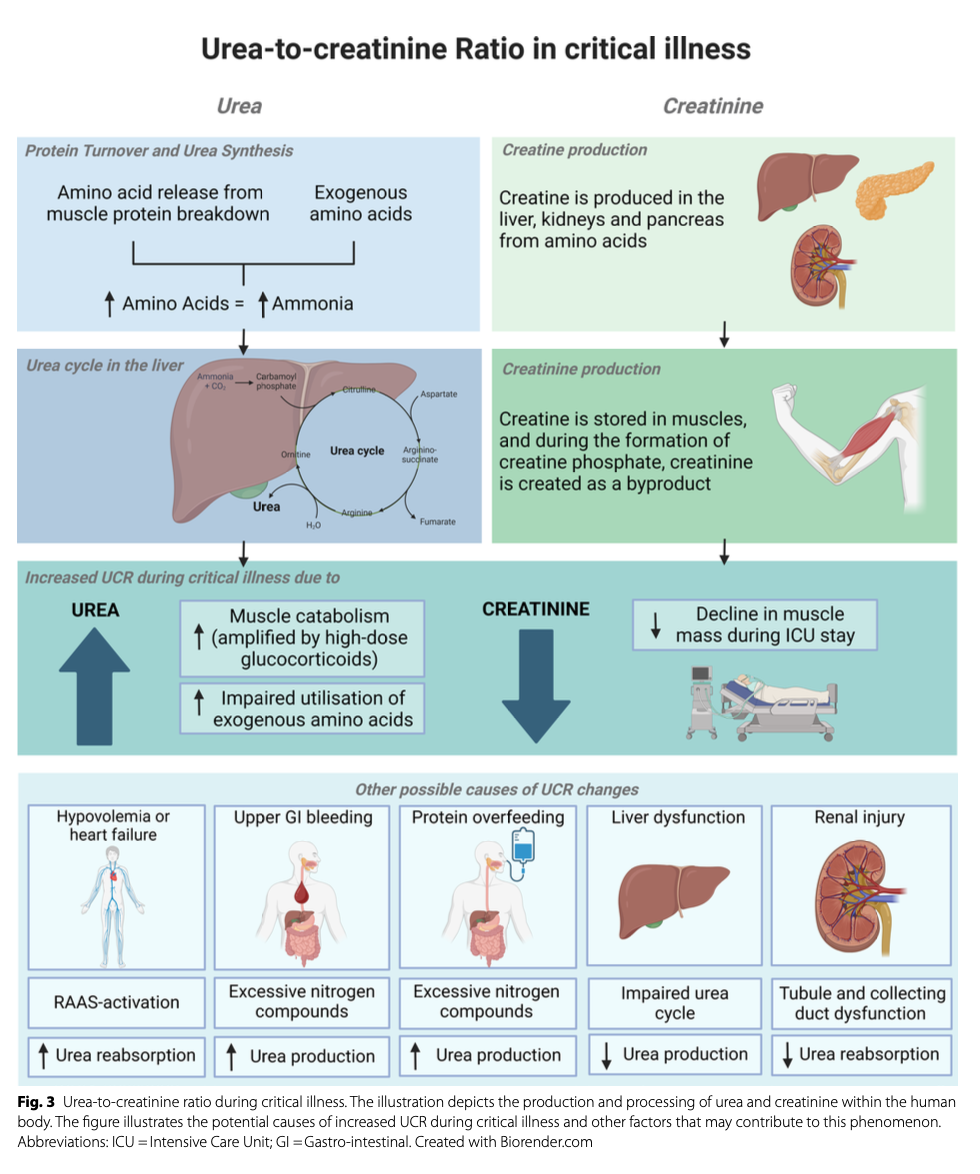
Discussion: UCR elevations during critical illness potentially indicate muscle protein catabolism and the progression to persistent critical illness, and high levels at ICU admission could be associated with mortality. UCR increments during ICU stay may also indicate excessive exogenous dietary protein intake, overwhelming the body’s ability to use it for whole-body or muscle protein synthesis. Dehydration, gastrointestinal bleeding, kidney and liver dysfunction, and renal replacement therapy may also influence UCR and are considered potential pitfalls when assessing catabolic phases of critical illness by UCR. Patient group-specific cut-off values are warranted to ensure its validity and application in clinical practice.
危重症期间UCR升高可能提示肌肉蛋白质分解代谢及向持续性危重症的进展,而ICU入院时UCR水平较高可能与死亡率相关。ICU住院期间UCR的升高也可能表明外源性膳食蛋白质摄入过多,超出了机体用于全身或肌肉蛋白质合成的能力。脱水、胃肠道出血、肾脏和肝脏功能障碍以及肾脏替代治疗也可能影响UCR,因此在利用UCR评估危重症的分解代谢阶段时,这些因素应被视为潜在的干扰因素。为确保UCR在临床实践中的有效性和适用性,有必要制定针对特定患者群体的临界值。
原创文章(本站视频密码:66668888),作者:xujunzju,如若转载,请注明出处:https://zyicu.cn/?p=20351
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫