Abstract
Background
The gray-white matter ratio (GWR) on head CT is a well-established marker of hypoxic-ischemic brain injury after cardiac arrest, but its prognostic performance may vary with the timing of imaging. We aimed (i) to evaluate the prognostic value of GWR across serial CT scans within the same comatose patients, and (ii) to determine whether the longitudinal changes of GWR provide additional prognostic information beyond single time-point measurements.头部CT上的灰质比(GWR)是心脏骤停后缺氧缺血性脑损伤公认的标志,但其预后表现可能因成像时间而异。我们的目的是(i)通过对同一昏迷患者的连续CT扫描来评估GWR的预后价值,以及(ii)确定GWR的纵向变化是否提供单一时间点测量之外的额外预后信息。
Methods
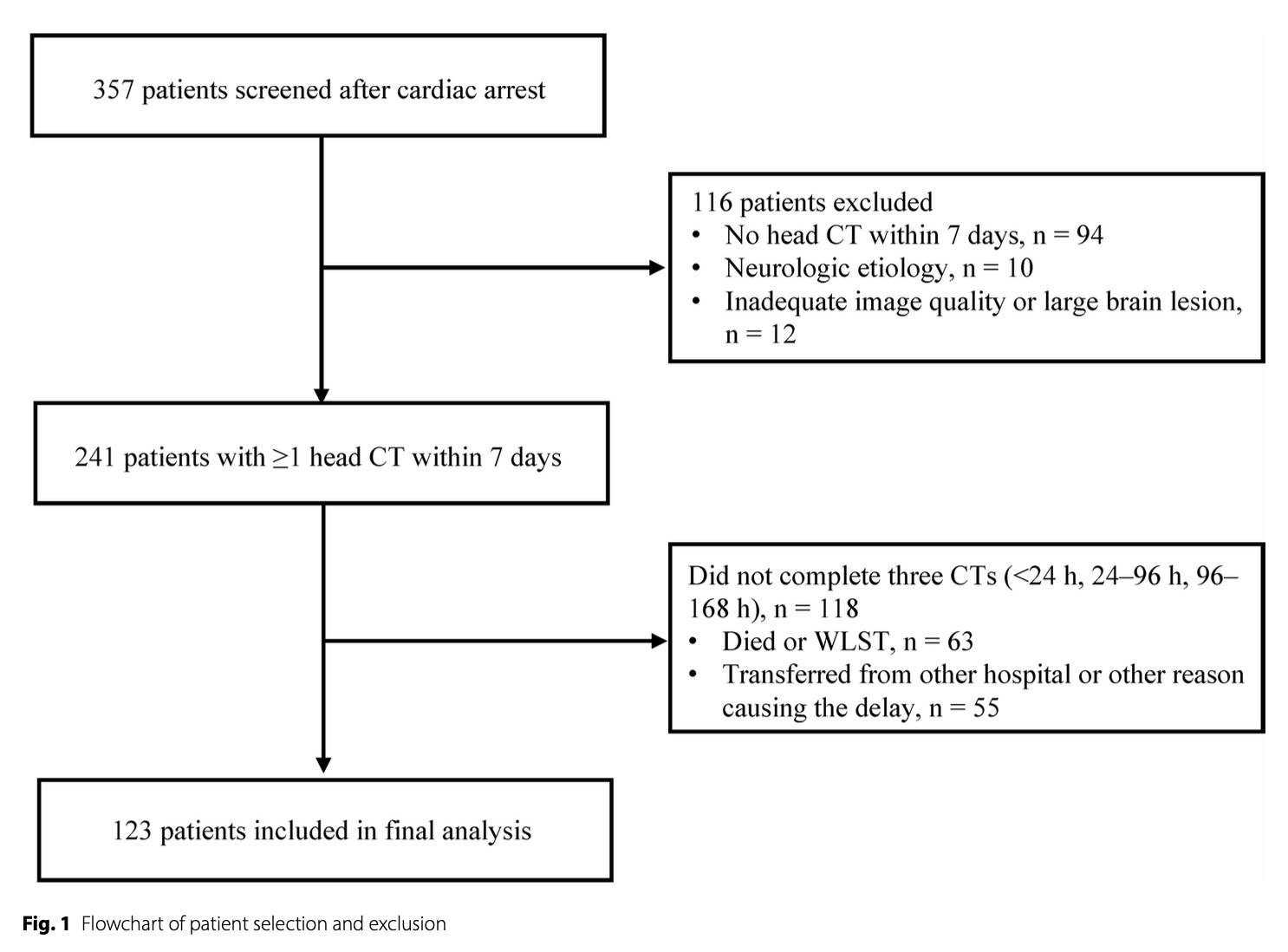
We prospectively recruited 123 comatose patients with cardiac arrest admitted to three intensive care units. All patients underwent serial non-contrast head CT at three predefined time windows (< 24 h, 24–96 h, and 96–168 h after cardiac arrest). GWR values were automatically calculated using an atlas-based approach. Neurological outcome at 3 months was assessed with the Cerebral Performance Category score (CPC) and dichotomized into good (CPC 1–2) or poor (CPC 3–5). GWR values and their progression were compared between outcome groups. Prognostic accuracy of GWR at each time window was assessed using receiver operating characteristic (ROC) analysis.我们前瞻性地招募了123名住在3个重症监护病房的心脏骤停昏迷患者。所有患者均在三个预定义的时间窗(心脏骤停后< 24小时、24 – 96小时和96-168小时)接受连续非对比头部CT检查。GWR值使用基于地图集的方法自动计算。用脑功能分类评分(CPC)评估3个月时的神经功能预后,并将其分为良好(CPC 1-2)或差(CPC 3 – 5)。结果组间比较GWR值及其进展。采用受试者工作特征(ROC)分析评估GWR在各时间窗的预后准确性。
Results
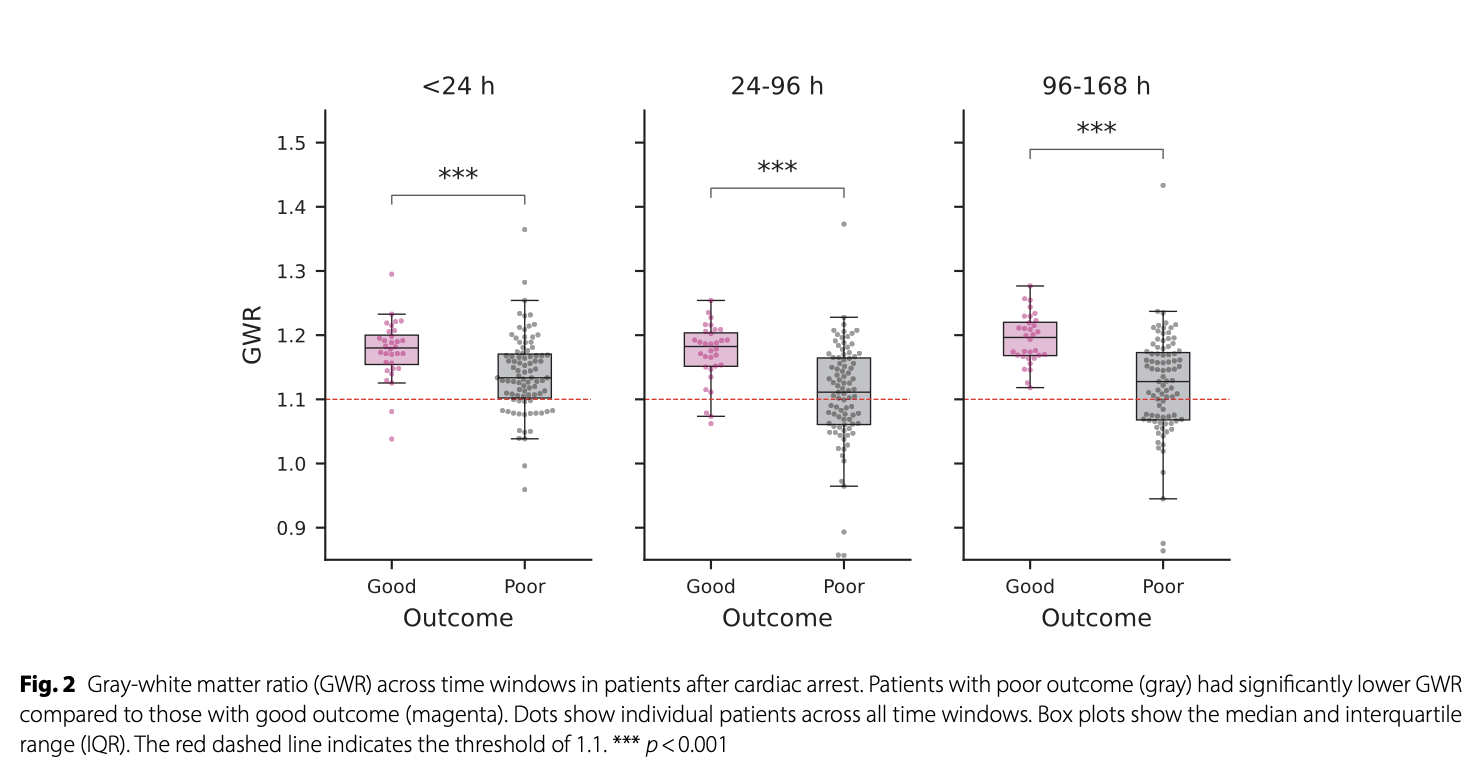
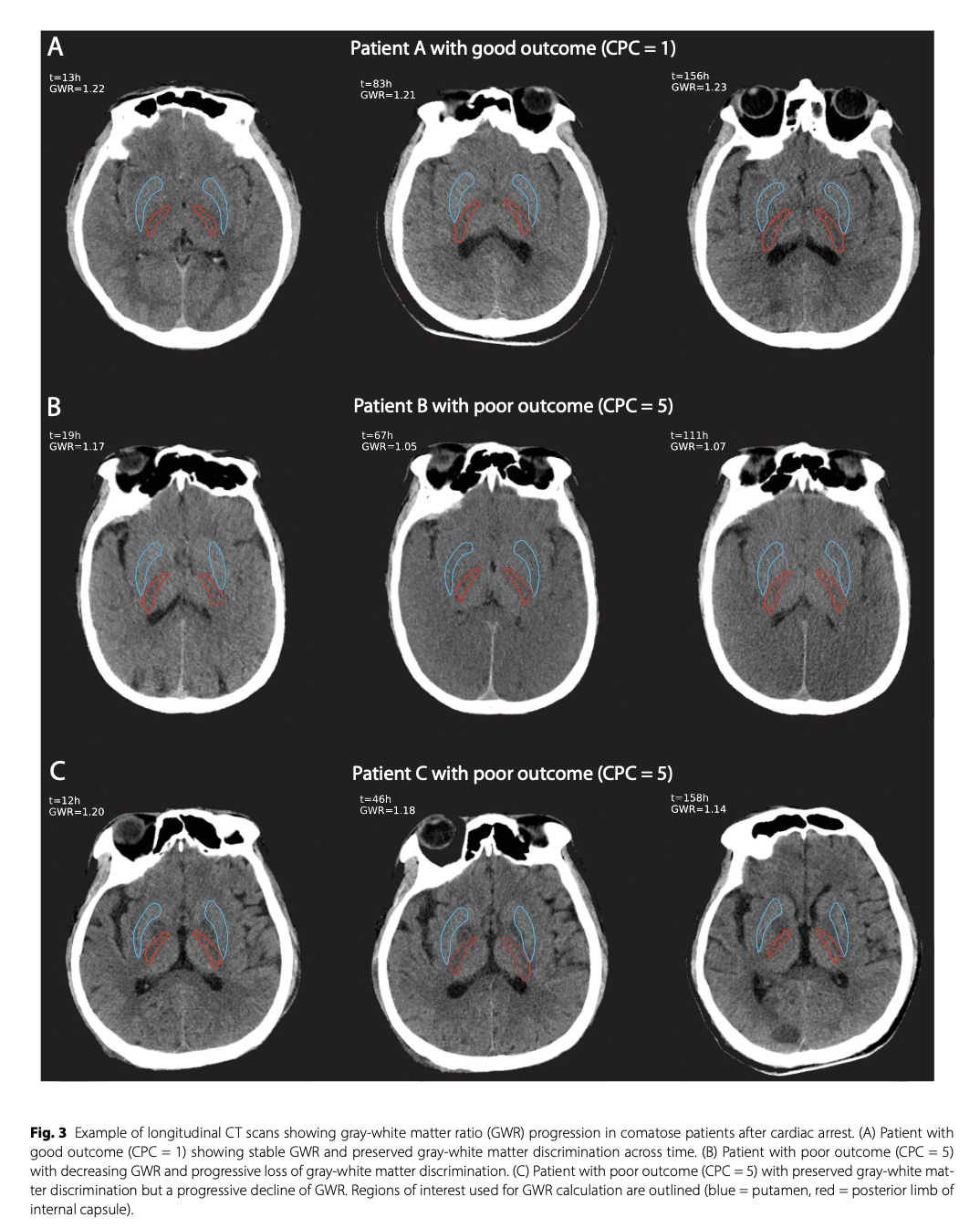
GWR was consistently lower in patients with poor outcomes compared to those with good outcomes across all time windows (for all p < 0.001). In poor-outcome patients, GWR declined after the first 24 h, whereas it was stable in good-outcome patients. The prognostic performance of GWR improved with later imaging, with an AUC of 0.72 (95% CI 0.62–0.81) at < 24 h, 0.78 (95% CI 0.69–0.86) at 24–96 h, and 0.81 (95% CI 0.72–0.88) at 96–168 h after cardiac arrest. Incorporating longitudinal changes in GWR slightly improved prediction, with the AUC increasing from 0.81 to 0.83 at 96–168 h.在所有时间窗口中,预后差的患者GWR始终低于预后好的患者(p < 0.001)。在预后差的患者中,GWR在24小时后下降,而在预后好的患者中则保持稳定。GWR的预后表现随着后期影像学的改善而改善,心脏骤停后< 24小时的AUC为0.72 (95% CI 0.62-0.81), 24 – 96小时的AUC为0.78 (95% CI 0.69-0.86), 96-168小时的AUC为0.81 (95% CI 0.72 – 0.88)。考虑GWR的纵向变化,预测结果略有改善,在96 ~ 168 h时AUC从0.81增加到0.83。
Conclusions
Automated GWR is a useful predictor of outcome after cardiac arrest, with higher accuracy on delayed CT (> 24 h). The different GWR progression trajectories between patients with poor and good outcomes suggest that longitudinal CT assessments may provide additional prognostic information.自动GWR是心脏骤停后预后的有效预测指标,在延迟CT(24小时)上具有更高的准确性。预后差和预后好的患者GWR的不同进展轨迹表明,纵向CT评估可以提供额外的预后信息。
原创文章(本站视频密码:66668888),作者:xujunzju,如若转载,请注明出处:https://zyicu.cn/?p=21443
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫