Abstract
Importance: Hypernatremia is common among hospitalized patients and is associated with high mortality rates. Current guidelines suggest avoiding fast correction rates but are not supported by robust data.
重要性:高钠血症在住院患者中较为常见,且与高死亡率相关。现行指南建议避免过快纠正血钠水平,但缺乏有力数据支持
Objective: To investigate whether there is an association between hypernatremia correction rate and patient survival.
目的:探讨高钠血症纠正速率与患者生存之间的关联。
Design, setting, and participants: This retrospective cohort study examined data from all patients admitted to the Tel Aviv Medical Center between 2007 and 2021 who were diagnosed with severe hypernatremia (serum sodium ≥155 mmol/L) at admission or during hospitalization. Statistical analysis was performed from April 2022 to August 2023.
设计、场所与参与者:本回顾性队列研究纳入了2007年至2021年间入住特拉维夫医疗中心的所有患者,其入院时或住院期间被诊断为重度高钠血症(血清钠≥155 mmol/L)。统计分析于2022年4月至2023年8月期间完成。
Exposure: Patients were grouped as having fast correction rates (>0.5 mmol/L/h) and slow correction rates (≤0.5 mmol/L/h) in accordance with current guidelines.
暴露因素:根据现行指南,将患者分为快速纠正组(纠正速率>0.5 mmol/L/h)和缓慢纠正组(纠正速率≤0.5 mmol/L/h)。
Main outcomes and measures: All-cause 30-day mortality.
主要结局与指标:全因30天死亡率。
Results: A total of 4265 patients were included in this cohort, of which 2621 (61.5%) were men and 343 (8.0%) had fast correction rates; the median (IQR) age at diagnosis was 78 (64-87) years. Slow correction was associated with higher 30-day mortality compared with fast correction (50.7% [1990 of 3922] vs 31.8% [109 of 343]; P < .001). These results remained significant after adjusting for demographics (age, gender), Charlson comorbidity index, initial sodium, potassium, and creatinine levels, hospitalization in an ICU, and severe hyperglycemia (adjusted odds ratio [aOR], 2.02 [95% CI, 1.55-2.62]), regardless of whether hypernatremia was hospital acquired (aOR, 2.19 [95% CI, 1.57-3.05]) or documented on admission (aOR, 1.64 [95% CI, 1.06-2.55]). There was a strong negative correlation between absolute sodium correction during the first 24 hours following the initial documentation of severe hypernatremia and 30-day mortality (Pearson correlation coefficient, -0.80 [95% CI, -0.93 to -0.50]; P < .001). Median (IQR) hospitalization length was shorter for fast correction vs slow correction rates (5.0 [2.1-14.9] days vs 7.2 [3.5-16.1] days; P < .001). Prevalence of neurological complications was comparable for both groups, and none were attributed to fast correction rates of hypernatremia.
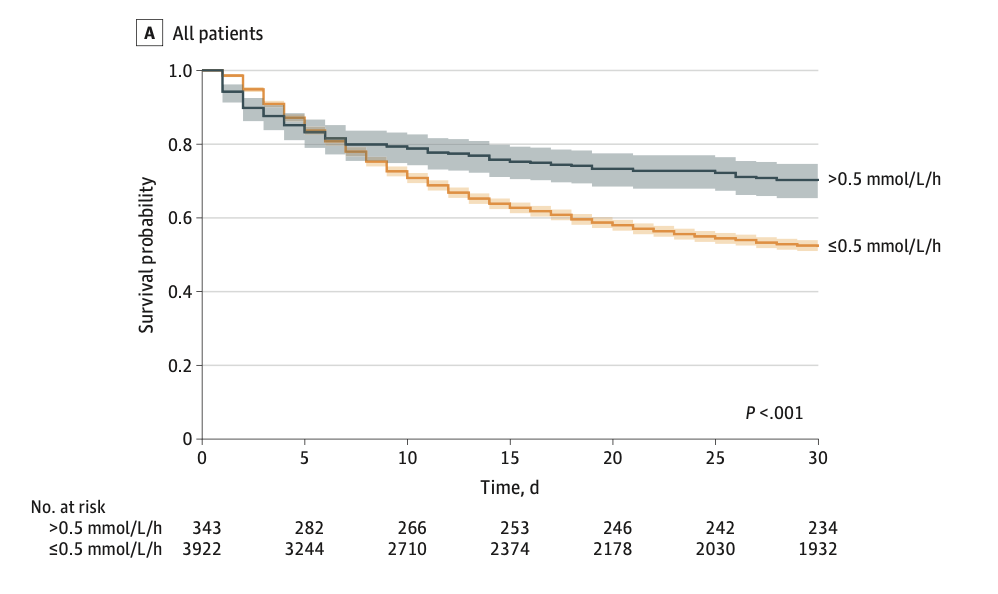
结果:共纳入4265例患者,其中男性2621例(61.5%),快速纠正者343例(8.0%);诊断时中位年龄(四分位距)为78(64-87)岁。与快速纠正相比,缓慢纠正与更高的30天死亡率相关(50.7% [3922例中1990例] vs 31.8% [343例中109例];P< 0.001)。调整人口学特征(年龄、性别)、查尔森合并症指数、初始钠/钾/肌酐水平、ICU住院史及严重高血糖后,上述差异仍显著(校正比值比[aOR] 2.02,95%置信区间[CI] 1.55-2.62);无论高钠血症是医院获得性(aOR 2.19,95%CI 1.57-3.05)还是入院时已存在(aOR 1.64,95%CI 1.06-2.55),结果均一致。重度高钠血症首次记录后24小时内血钠绝对纠正量与30天死亡率呈强负相关(皮尔逊相关系数-0.80,95%CI -0.93至-0.50;P< 0.001)。快速纠正组的住院时长中位值(四分位距)短于缓慢纠正组(5.0 [2.1-14.9]天 vs 7.2 [3.5-16.1]天;P< 0.001)。两组神经并发症发生率相当,且无病例归因于高钠血症的快速纠正。
Conclusions and relevance: This cohort study of patients with severe hypernatremia found that rapid correction of hypernatremia was associated with shorter hospitalizations and significantly lower patient mortality without any signs of neurologic complications. These results suggest that physicians should consider the totality of evidence when considering the optimal rates of correction for patients with severe hypernatremia
结论与相关性:这项针对重度高钠血症患者的队列研究发现,快速纠正高钠血症与更短的住院时间及显著降低的患者死亡率相关,且未观察到神经并发症迹象。这些结果表明,临床医生在制定重度高钠血症最佳纠正速率时,应综合考虑现有全部证据。
原创文章(本站视频密码:66668888),作者:xujunzju,如若转载,请注明出处:https://zyicu.cn/?p=21531
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫