ABSTRACT
BACKGROUND
Myocardial infarction is a frequent cause of out-of-hospital cardiac arrest. However, the benefits of early coronary angiography and revascularization in resuscitated patients without electrocardiographic evidence of ST-segment elevation are unclear. 心肌梗死是院外心脏停搏的常见原因。然而,对于心电图无ST段抬高的心肺复苏成功患者,早期冠状动脉造影和血运重建的益处尚未明确。
METHODS
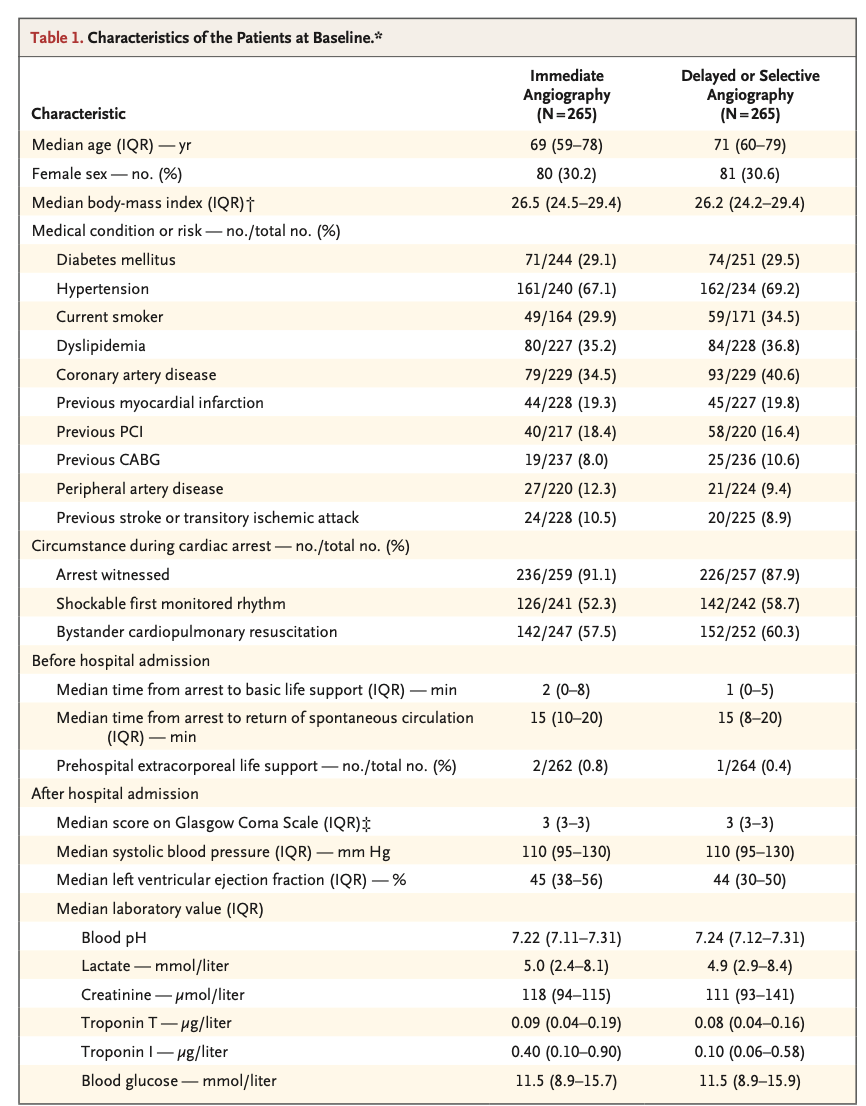
In this multicenter trial, we randomly assigned 554 patients with successfully resuscitated out-of-hospital cardiac arrest of possible coronary origin to undergo either immediate coronary angiography (immediate-angiography group) or initial intensive care assessment with delayed or selective angiography (delayed-angiography group). All the patients had no evidence of ST-segment elevation on postresuscitation electrocardiography. The primary end point was death from any cause at 30 days. Secondary end points included a composite of death from any cause or severe neurologic deficit at 30 days. 在此项多中心试验中,我们将554例可能由冠状动脉事件导致的院外心脏停搏并且心肺复苏成功的患者随机分组,两组分别接受即刻冠状动脉造影(即刻造影组)或初始重症监护评估联合延迟或选择性冠状动脉造影(延迟造影组)。所有患者在心肺复苏成功后的心电图上均无ST段抬高。主要终点是30日内的全因死亡。次要终点是由30日内的全因死亡或重度神经功能缺损构成的复合终点。
RESULTS
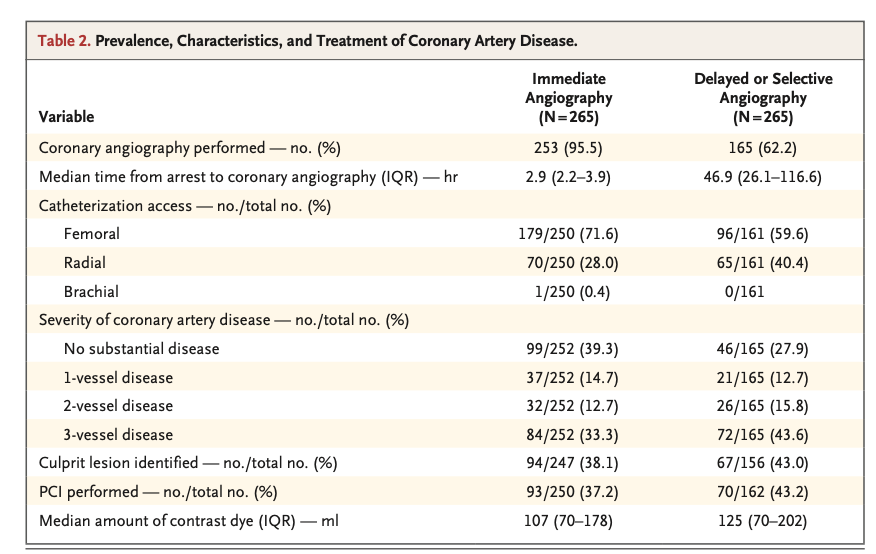
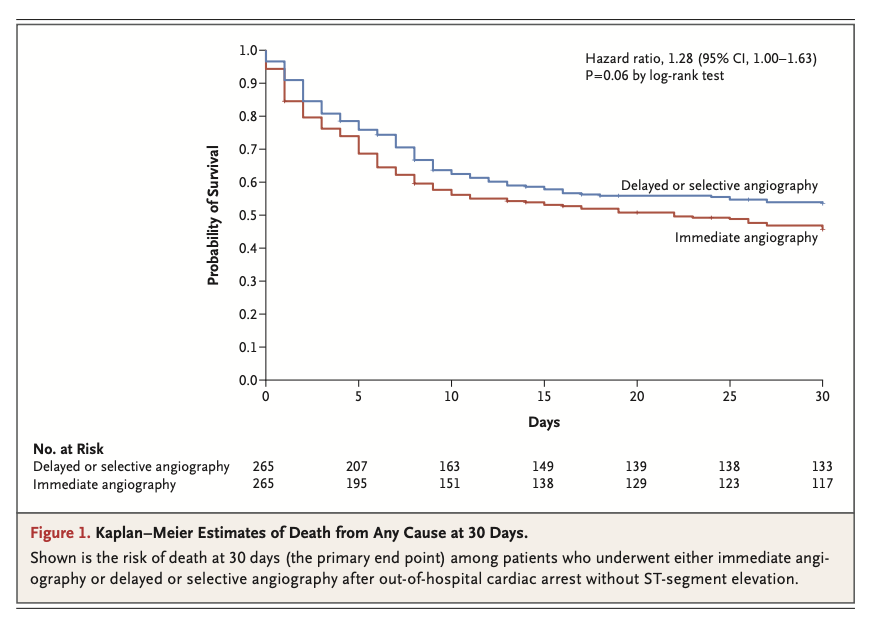
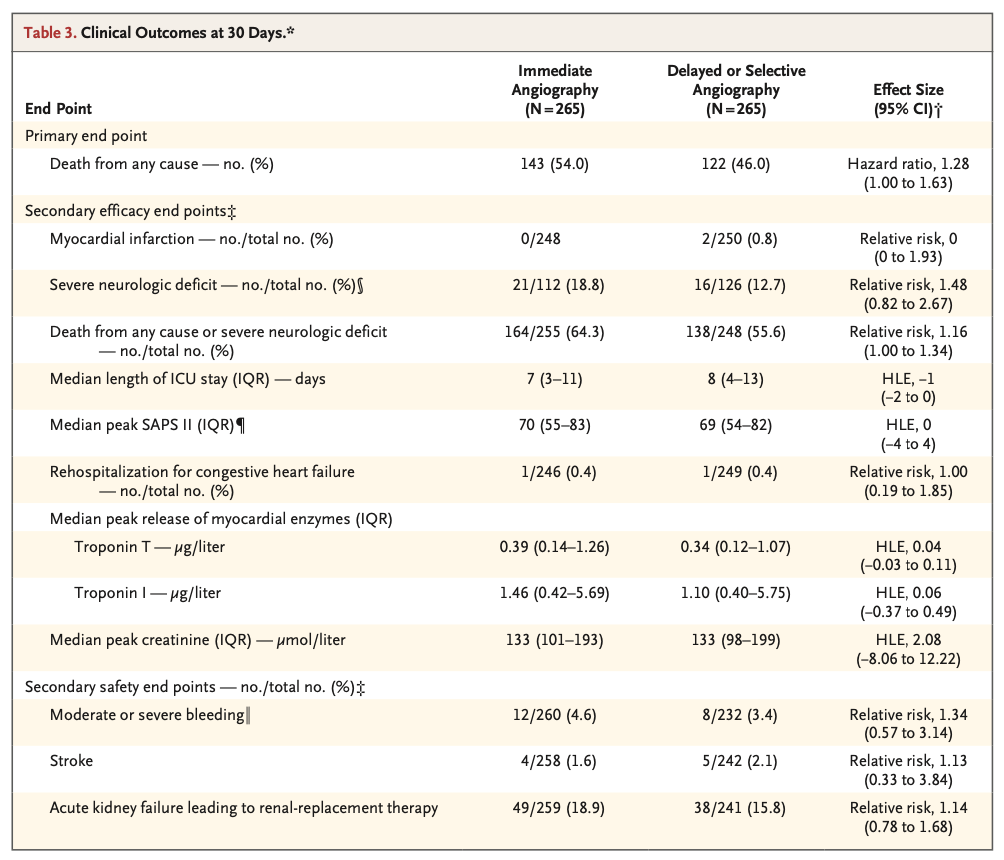
A total of 530 of 554 patients (95.7%) were included in the primary analysis. At 30 days, 143 of 265 patients (54.0%) in the immediate-angiography group and 122 of 265 patients (46.0%) in the delayed-angiography group had died (hazard ratio, 1.28; 95% confidence interval [CI], 1.00 to 1.63; P=0.06). The composite of death or severe neurologic deficit occurred more frequently in the immediate-angiography group (in 164 of 255 patients [64.3%]) than in the delayed-angiography group (in 138 of 248 patients [55.6%]), for a relative risk of 1.16 (95% CI, 1.00 to 1.34). Values for peak troponin release and for the incidence of moderate or severe bleeding, stroke, and renal-replacement therapy were similar in the two groups. 554例患者中有530例(95.7%)被纳入主要分析。在第30日,即刻造影组265例患者中的143例(54.0%)和延迟造影组265例患者中的122例(46.0%)已死亡(风险比,1.28;95% CI,1.00~1.63;P=0.06)。即刻造影组(255例患者中的164例[64.3%])中,由死亡或重度神经功能缺损构成的复合终点的发生率高于延迟造影组(248例患者中的138例[55.6%]),相对危险度为1.16(95% CI,1.00~1.34)。两组的肌钙蛋白释放峰值及中度或重度出血、卒中和肾脏替代治疗的发生率相似。
CONCLUSIONS
Among patients with resuscitated out-of-hospital cardiac arrest without ST-segment elevation, a strategy of performing immediate angiography provided no benefit over a delayed or selective strategy with respect to the 30-day risk of death from any cause. (Funded by the German Center for Cardiovascular Research; TOMAHAWK ClinicalTrials.gov number, NCT02750462.) 在院外心脏停搏后复苏成功且无ST段抬高的患者中,在30日内的全因死亡风险方面,即刻造影策略并不优于延迟或选择性造影策略(由德国心血管研究中心[German Center for Cardiovascular Research]资助,TOMAHAWK在ClinicalTrials.gov注册号为NCT02750462)。
全部翻译请查看nejm医学前沿院外心脏停搏后无ST段抬高患者的血管造影。
特别申明:本文为转载文章,转载自nejm医学前沿,不代表贪吃的夜猫子立场,如若转载,请注明出处:https://nejmqianyan.cn/article-info?permalinks=YXQYoa2101909&sg=AbW1NGsHw3NxPd6F
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫