Introduction
Extracorporeal cardiopulmonary resuscitation (ECPR) is a critical rescue strategy for refractory out-of-hospital cardiac arrest (OHCA), but its success is highly dependent on patient selection and timely initiation [1]. Older age and prolonged extracorporeal membrane oxygenation (ECMO) initiation time are known to negatively affect outcomes [2, 3]. Guidelines recommend initiating ECMO within 60 min of cardiac arrest, and experts advocate for early consideration of ECPR [1]. Despite these recommendations, the upper time limit for ECPR effectiveness remains uncertain, particularly in older OHCA patients. This study aims to define the upper limit for ECPR initiation time and investigate how advanced age influences this threshold.体外心肺复苏(ECPR)是治疗难治性院外心脏骤停(OHCA)的关键急救策略,但其成功率高度依赖于患者的选择和及时的启动[1]。已知高龄和体外膜肺氧合(ECMO)启动时间过长会对预后产生不利影响[2, 3]。指南建议在心脏骤停后60分钟内启动ECMO,专家也提倡尽早考虑ECPR[1]。尽管有这些建议,但ECPR有效性的时间上限仍不明确,尤其是在高龄OHCA患者中。本研究旨在确定ECPR启动时间的上限,并探究高龄如何影响这一阈值。
Methods
We conducted a retrospective cohort study using data from the nationwide Korean OHCA database from 2016 to 2021. The database systematically records consecutive adult OHCA cases attended by emergency medical services (EMS) following standardized Utstein guidelines. The study included 483 adult (≥ 18 years) patients who received ECPR for non-traumatic OHCA. ECPR initiation time was defined as the time from hospital arrival to ECMO pump-on time. The primary outcome was a survival-to-discharge rate. The Institutional Review Board of Asan Medical Center granted ethical approval with a waiver for informed consent (IRB No. 2023–0438).我们使用2016至2021年韩国全国OHCA数据库的数据进行了一项回顾性队列研究。该数据库按照标准化的Utstein指南,系统记录了由急救医疗服务(EMS)接诊的连续成年OHCA病例。研究纳入了483名接受ECPR治疗的非创伤性OHCA成年患者(年龄≥18岁)。ECPR启动时间定义为从患者到达医院到ECMO泵启动的时间。主要结局是出院存活率。峨山医疗中心机构审查委员会批准了该研究并豁免了知情同意(伦理审批号:2023 – 0438)。
Patients were stratified into two groups: elderly (age > 65 years, n = 104) and non-elderly (age ≤ 65 years, n = 379). We used multivariable logistic regression to assess the effects of age, ECPR initiation time, and their interaction on survival. Variables included in the multivariable model were selected based on clinical relevance and variance inflation factor < 10. Dynamic and cumulative survival proportions were used to identify time thresholds [4].我们将患者分为两组:高龄组(年龄>65岁,n = 104)和非高龄组(年龄≤65岁,n = 379)。我们采用多变量逻辑回归分析来评估年龄、ECPR启动时间及其相互作用对存活率的影响。多变量模型中纳入的变量是基于临床相关性和方差膨胀因子<10来选择的。我们使用动态和累积存活比例来确定时间阈值[4]。
Results
Age distribution for elderly (> 65 years) and non-elderly (≤ 65 years) patients is presented in Supplementary Fig. 1. The median (interquartile range) age was 70.0 (68.0–74.0) years in the elderly group and 52.0 (44.0–60.0) years in the non-elderly group.高龄组(>65岁)和非高龄组(≤65岁)患者的年龄分布见补充图1。高龄组的中位(四分位数间距)年龄为70.0(68.0 – 74.0)岁,非高龄组为52.0(44.0 – 60.0)岁。
The overall survival-to-discharge rate was 18.2% (88 of 483 patients). After adjusting for confounding variables, both increasing age (adjusted OR: 0.97, 95% CI: 0.95–0.99, P < 0.001) and longer ECPR initiation time (adjusted OR: 0.97, 95% CI: 0.95–0.98, P = 0.003) were independently associated with decreased survival. A significant interaction was found between age and initiation time (adjusted OR: 0.999, 95% CI: 0.998–1.000, P = 0.021), indicating that treatment delays have a more pronounced negative effect on older patients (Supplemental eTable1).总体出院存活率为18.2%(483名患者中有88名)。在调整混杂变量后,年龄增长(调整后的比值比:0.97,95%置信区间:0.95 – 0.99,P<0.001)和ECPR启动时间延长(调整后的比值比:0.97,95%置信区间:0.95 – 0.98,P = 0.003)均与存活率降低独立相关。年龄和启动时间之间存在显著的交互作用(调整后的比值比:0.999,95%置信区间:0.998 – 1.000,P = 0.021),这表明治疗延迟对高龄患者的负面影响更为显著(补充电子表1)。
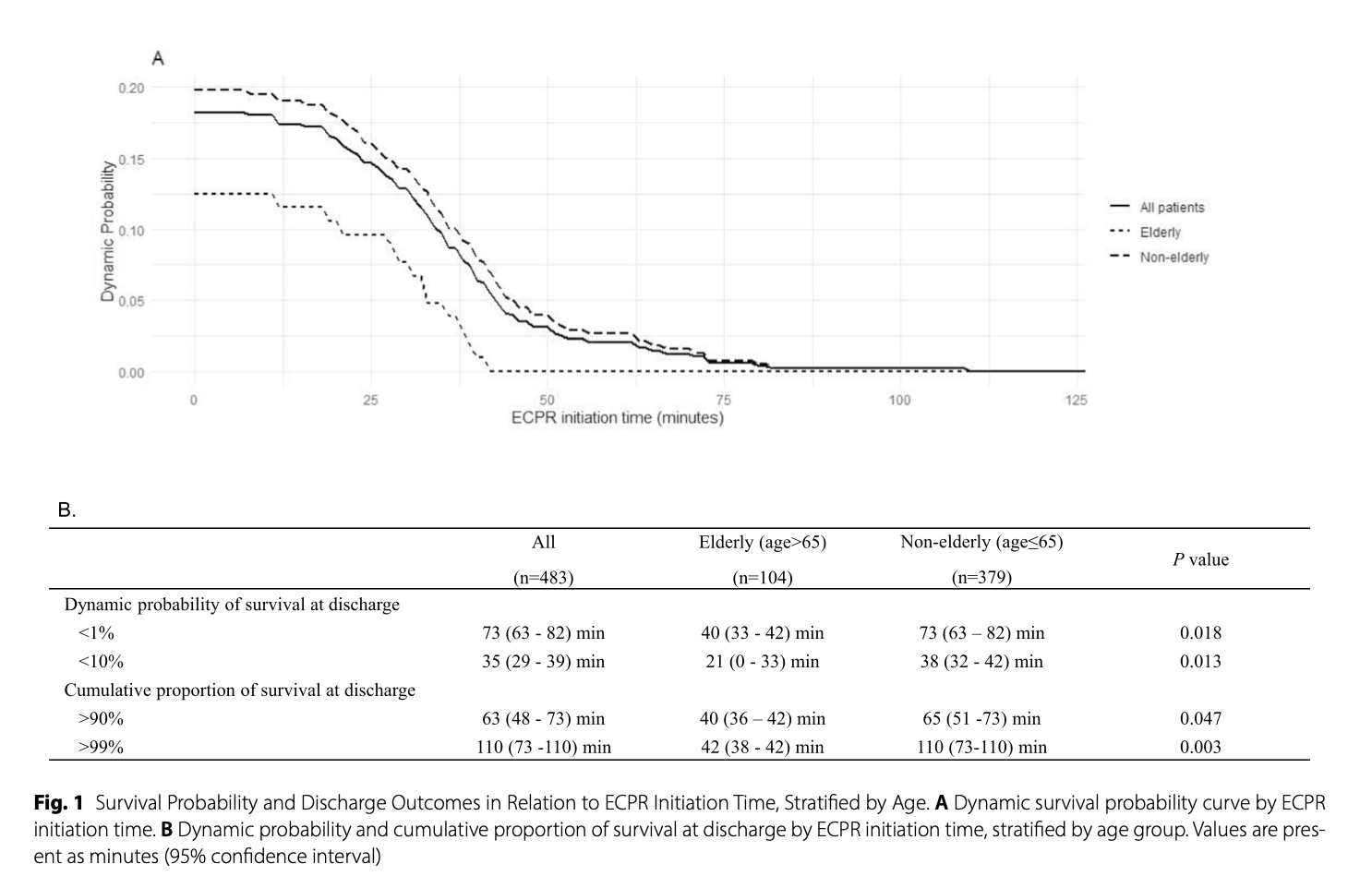
Age-stratified analysis revealed significantly different time windows for effective treatment (Fig. 1). In elderly patients, the probability of survival dropped below 10% when ECPR initiation was delayed beyond 21 (0–33 min) minutes, and it fell below 1% after 40 min (33–42 min). In contrast, non-elderly patients maintained a 10% survival probability for up to 38 min (32–42 min) and a 1% probability for up to 73 min (63–82 min) of initiation time. The ECPR time threshold difference between groups was statistically significant. The cumulative survival rate reached 90% after 40 min of CPR in elderly patients and 65 min in non-elderly patients.按年龄分层分析显示,有效治疗的时间窗存在显著差异(图1)。在高龄患者中,当ECPR启动延迟超过21(0 – 33)分钟时,存活概率降至10%以下,在40分钟(33 – 42)后降至1%以下。相比之下,非高龄患者在启动时间为38分钟(32 – 42)内可保持10%的存活概率,在73分钟(63 – 82)内可保持1%的存活概率。两组之间的ECPR时间阈值差异具有统计学意义。高龄患者在心肺复苏(CPR)40分钟后累积存活率达到90%,非高龄患者在65分钟后达到90%。
Discussion
This study demonstrates that both ECPR initiation time and age are independent predictors of survival to discharge in OHCA patients. Elderly patients showed a markedly reduced survival probability when ECMO initiation was delayed beyond 21 min, whereas non-elderly patients maintained higher survival potential until much later time points. These findings emphasize the need for more rapid ECPR initiation in elderly individuals.本研究表明,ECPR启动时间和年龄都是OHCA患者出院存活率的独立预测因素。高龄患者在ECMO启动延迟超过21分钟时,存活概率显著降低,而非高龄患者在更晚的时间点仍能保持较高的存活可能性。这些发现强调了在高龄患者中更快启动ECPR的必要性。
Consistent with previous literature, our results confirm the inverse relationship between ECPR initiation time and survival outcomes. While current guidelines recommend ECMO initiation within 60 min [1], our data suggest that this threshold may be too long for elderly patients. Notably, survival remained possible up to 110 min of CPR in non-elderly patients, but the effective therapeutic window was significantly shorter in the elderly. This age-dependent benefit underscores the importance of timely decision-making tailored to patient age.与以往文献一致,我们的结果证实了ECPR启动时间和生存结局之间的负相关关系。虽然现行指南建议在60分钟内启动ECMO[1],但我们的数据表明,对于高龄患者来说,这一阈值可能过长。值得注意的是,非高龄患者在CPR 110分钟内仍有可能存活,但高龄患者的有效治疗时间窗明显更短。这种与年龄相关的益处凸显了根据患者年龄及时做出决策的重要性。
ECPR initiation time may serve as a practical surrogate for low-flow duration, which is often difficult to quantify during resuscitation [3, 5]. As such, ECPR timing could represent a more feasible quality metric for clinical decision-making, reflecting team readiness and system efficiency. Given the sharp decline in survival beyond 20 min in the elderly, early ECPR activation—ideally within 20 min—should be considered in carefully selected candidates.ECPR启动时间可以作为低流量持续时间的实用替代指标,而低流量持续时间在复苏过程中往往难以量化[3, 5]。因此,ECPR启动时间可能是一个更可行的临床决策质量指标,能反映团队的准备情况和系统的效率。鉴于高龄患者在20分钟后存活率急剧下降,对于经过精心筛选的患者,应考虑尽早(理想情况下在20分钟内)启动ECPR。
This study has limitations inherent to its retrospective design, including potential selection bias, limited information on CPR quality, and differences in post-resuscitation care. Additionally, generalizability may be restricted to other healthcare systems. Nonetheless, the large-scale, standardized registry data provide meaningful insights into age-specific timing strategies for ECPR implementation in OHCA.本研究存在回顾性设计固有的局限性,包括潜在的选择偏倚、关于CPR质量的有限信息以及复苏后护理的差异。此外,研究结果的普遍性可能仅适用于其他医疗系统。尽管如此,大规模、标准化注册数据为OHCA中ECPR实施的年龄特异性时间策略提供了有意义的见解。
In conclusion, the effective time window for ECPR is significantly shorter in elderly patients. To maximize the potential for survival in this group, clinical teams must make rapid decisions and mobilize for ECPR initiation almost immediately upon patient arrival, ideally within 20 min.总之,高龄患者的ECPR有效时间窗明显更短。为了最大化这一群体的存活可能性,临床团队必须在患者到达后几乎立即快速做出决策并启动ECPR,理想情况下应在20分钟内完成。
原创文章(本站视频密码:66668888),作者:xujunzju,如若转载,请注明出处:https://zyicu.cn/?p=20804
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫