Background
Recent medical society opinions have questioned the use of early antimicrobials in patients with sepsis, but without septic shock. 最近的医学社会关于对脓毒症但无脓毒性休克患者早期抗菌药的使用提出了质疑。
Research Question
Is time from ED presentation to administration of antibiotics associated with progression to septic shock among patients with suspected infection? 在疑似感染的患者中,从前往ED就诊至抗生素给药的时间是否与进展为脓毒性休克相关?
Study Design and Methods
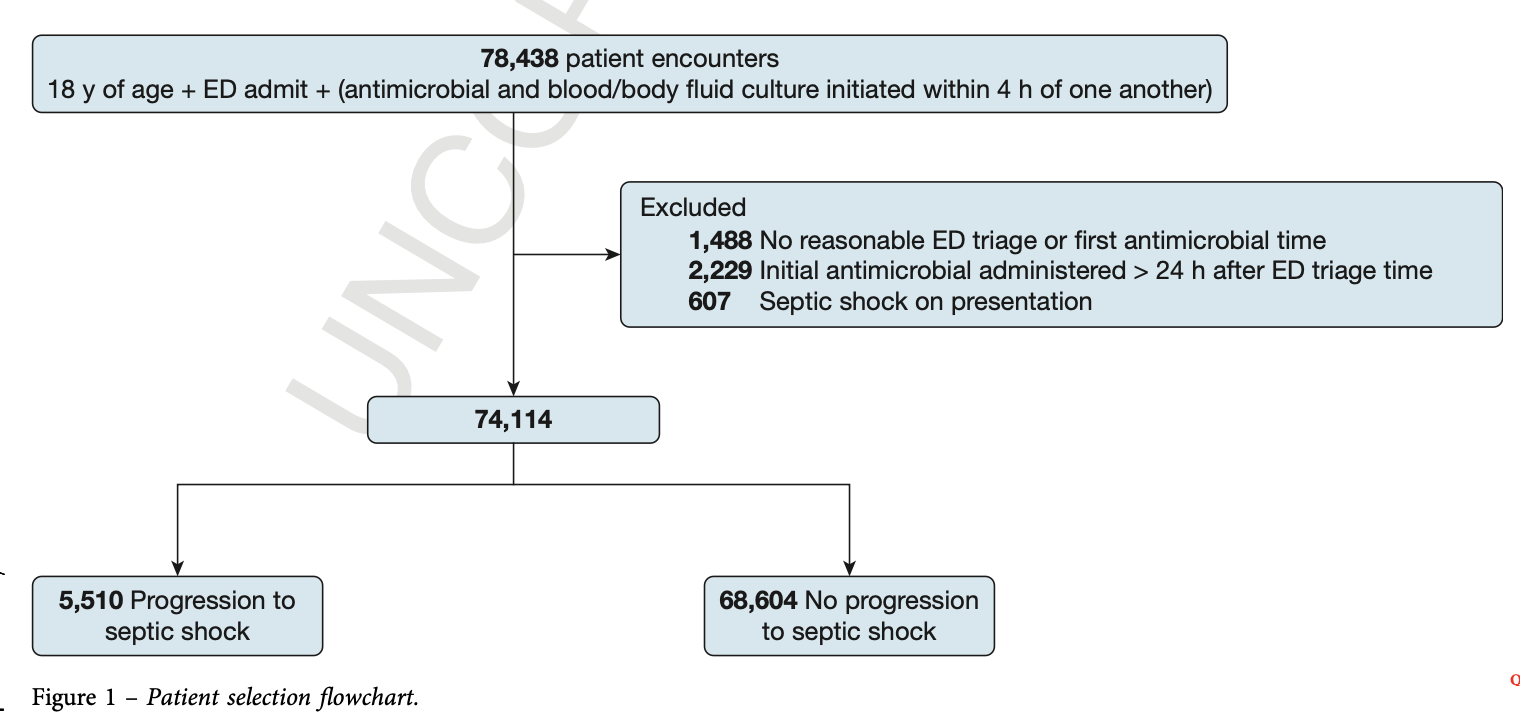
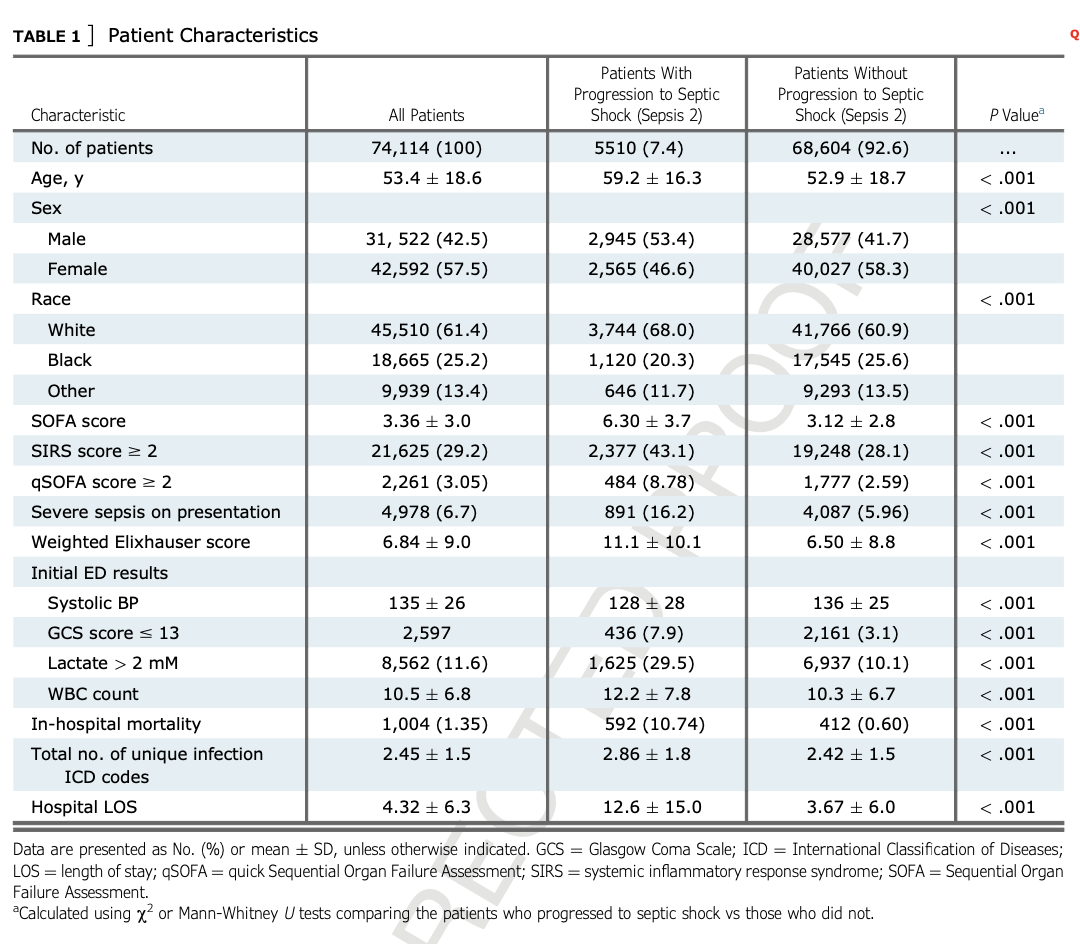
This was a retrospective cohort study from March 2007 through March 2020. All adults with suspected infection and first antimicrobial administered within 24 h of triage were included. Patients with shock on presentation were excluded. We performed univariate and multivariate logistic regression analyses predicting progression to septic shock. 这是一项2007年3月至2020年3月的回顾性队列研究。纳入所有疑似感染且在分诊24 h内首次给予抗菌药物的成人患者。排除就诊时就有休克的患者。我们进行了单变量和多变量logistic回归分析用以预测是否进展为感染性休克。
Results
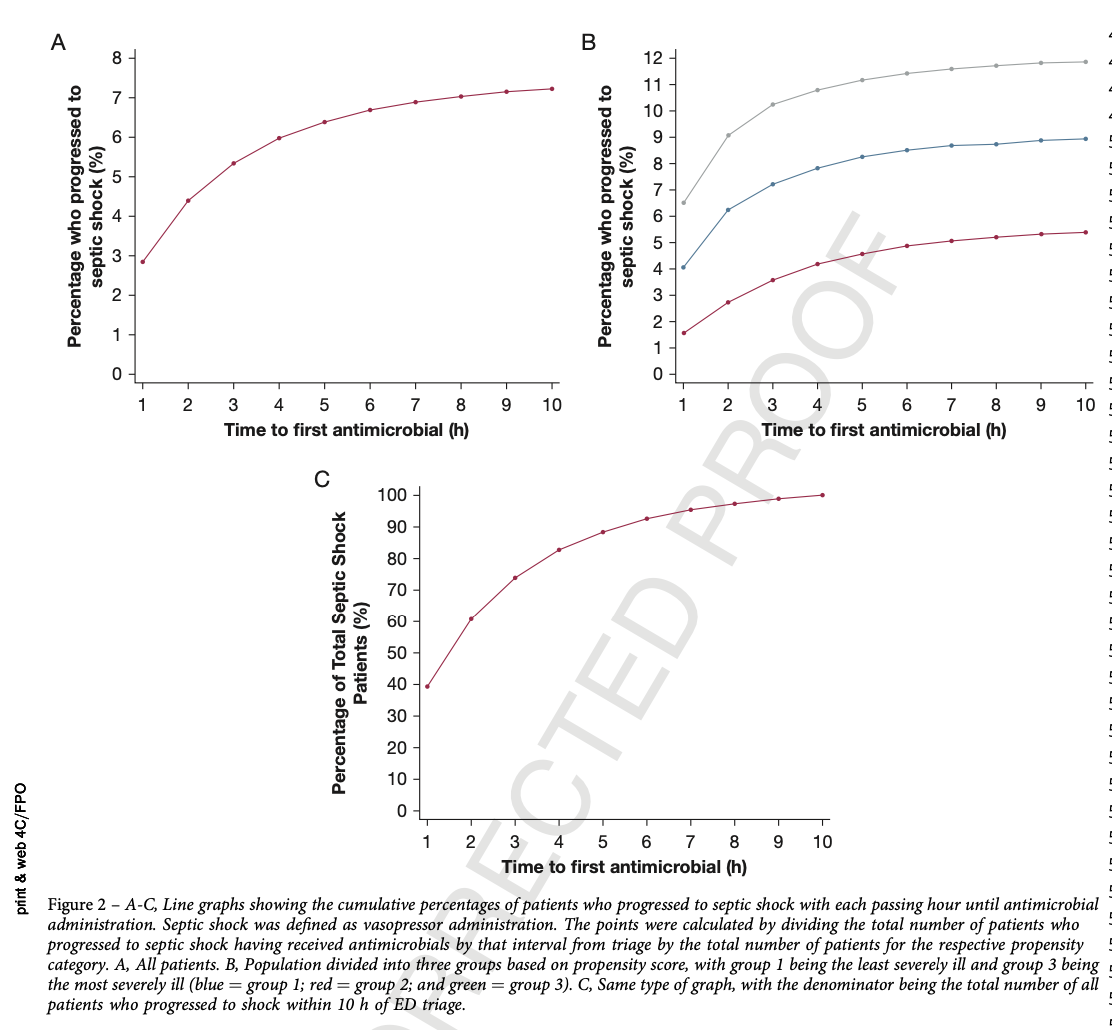
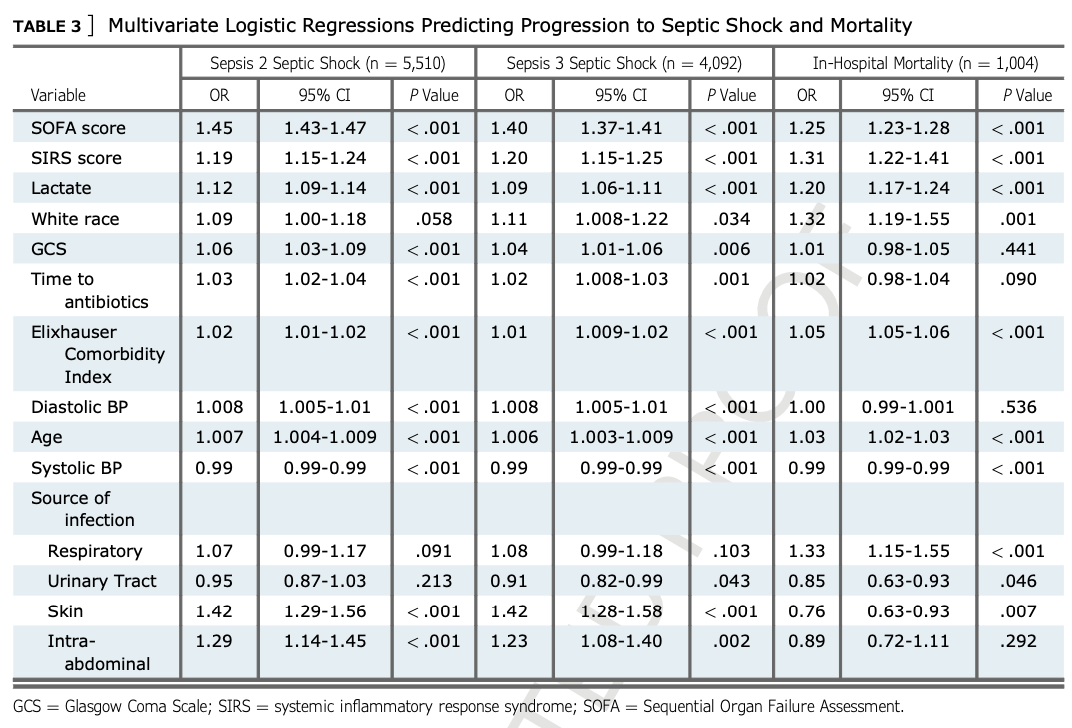
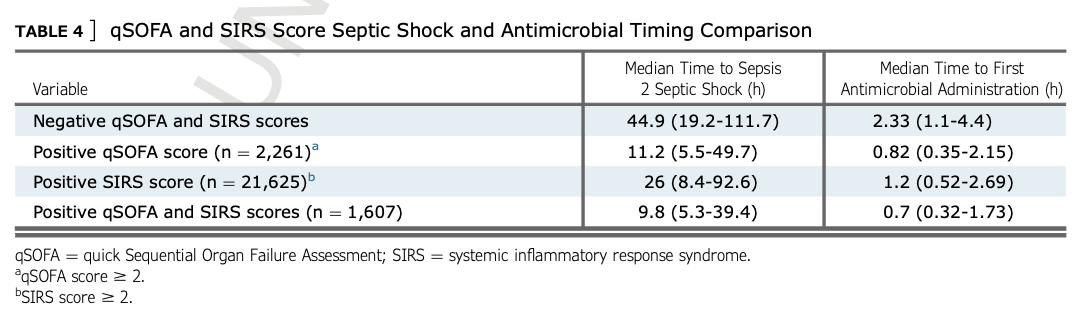
Seventy-four thousand one hundred fourteen patient encounters were included in the study. Five thousand five hundred ten patients (7.4%) progressed to septic shock. Of the patients who progressed to septic shock, 88% had received antimicrobials within the first 5 h from triage. In the multivariate logistic model, time (in hours) to first antimicrobial administration showed an OR of 1.03 (95% CI, 1.02-1.04; P < .001) for progression to septic shock and 1.02 (95% CI, 0.99-1.04; P = .121) for in-hospital mortality. When adjusted for severity of illness, each hour delayed until initial antimicrobial administration was associated with a 4.0% increase in progression to septic shock for every 1 h up to 24 h from triage. Patients with positive quick Sequential Organ Failure Assessment (qSOFA) results were given antibiotics at an earlier time point than patients with positive systemic inflammatory response syndrome (SIRS) score (0.82 h vs 1.2 h; P < .05). However, median time to septic shock was significantly shorter (P < .05) for patients with positive qSOFA results at triage (11.2 h) compared with patients with positive SIRS score at triage (26 h). 本研究纳入了74114例患者。其中5510例患者(7.4%)进展为脓毒性休克。在进展为感染性休克的患者中,88%在分诊后的前5 h内接受过抗菌药治疗。在多变量logistic模型中,至首次抗菌药物给药的时间(小时)显示OR为1.03(95%CI,1.02-1.04;P < .001)和1.02(95%CI,0.99-1.04;P = .121)的住院死亡率。当调整疾病的严重程度时,延迟初始抗菌药物给药的每一小时与从分诊开始每1h直至24h进展为感染性休克增加4.0%相关。快速序贯器官衰竭评估(qSOFA)结果阳性的患者比全身炎症反应综合征(SIRS)评分阳性的患者在更早的时间点给予抗生素(0.82h vs 1.2h;P < .05).然而,与分诊时SIRS评分阳性的患者(26h)比较,分诊时qSOFA结果阳性的患者(11.2h)组感染性休克的中位时间显著缩短(P < .05)。
Interpretation
Delays in first antimicrobial administration in patients with suspected infection are associated with rapid increases in likelihood of progression to septic shock. Additionally, qSOFA score has higher specificity than SIRS score for predicting septic shock, but is associated with a worse outcome, even when patients receive early antibiotics. 疑似感染患者首次抗菌药物给药延迟与进展为脓毒性休克的可能性迅速增加相关。此外,qSOFA评分在预测感染性休克方面比SIRS评分具有更高的特异性,但与更差的结果相关,即使患者接受早期接受抗生素。
原创文章(本站视频密码:66668888),作者:xujunzju,如若转载,请注明出处:https://zyicu.cn/?p=9523
 微信扫一扫
微信扫一扫  支付宝扫一扫
支付宝扫一扫